

- Breaking News
- April 8, 2024
- 51 views
- 9 minutes Read
English News: Actually, It’s OK to Slouch
English News: Actually, It’s OK to Slouch
[[{“value”:”
One of the latest and surprising findings in the field of physical therapy is that slouching is not as bad as we think it is. Certain researchers have gone so far as to say that the conventional fear mongering regarding poor posture can actually be more harmful than slouching itself. Undoing over a century’s worth of public health messaging about the evils of poor posture—let alone the custom of elders telling youngsters to “sit up straight”—will be a monumental task.
[time-brightcove not-tgx=”true”]
I know because I’ve spent the better part of a decade researching the so-called “poor posture epidemic” of the 20th century, studying the myriad ways in which posture panic has become part of the fabric of our everyday lives. What I’ve found is that some of our most cherished beliefs about posture health are unexamined remnants of cultural and political concerns from the past.
At the turn of the century, the idea that poor posture posed a serious population-wide health threat became entrenched in American public and popular health culture, thanks in part to the then-burgeoning fields of evolutionary medicine and paleoanthropology. Applying the theories of Charles Darwin to medical practice, early posture advocates such as Jessie H. Bancroft, R. Tait McKenzie, and Eliza M. Mosher—founders of the American Posture League –began to argue that without proper preventative health treatment, bipedalism might actually be an inherent weakness to human functioning, causing organ prolapses and other musculoskeletal problems not found among quadrupedal non-human animals.
The first study to report on the extent of the problem—the 1917 “Harvard Slouch” study – found that 80% of Americans had bad posture. This spurred further nationwide studies at universities, workplaces, and within the military for much of the twentieth century, all of which came to a similar conclusion. Along the way, industrialists learned that the poor posture epidemic was good for business, leading to new, lucrative markets in ergonomic chairs, back braces, shoes, and fitness regimes, such as yoga and Pilates.
By the mid 20th century, poor posture came to be seen as the culprit for rising rates of low back pain, even though little hard evidence existed to prove such claims of causality. President John F. Kennedy, who had repeated back surgeries and chronic pain, hired his own personal posture guru, Hans Kraus, a man who would go on to create one of the most well-known posture and fitness tests administered to hundreds of thousands public school children throughout the Cold War. It was in this cultural and political context of containment that uprightness became a symbol of patriotism, heterosexual propriety, and individualist strength, all virtues believed to be needed in order to defeat the threat of communism.
And yet even after the Cold War came to an end, the belief in the causality between poor posture and future ill health remained largely unquestioned .
Today, epidemiologists estimate that approximately 568.4 million cases of disabling low back pain exist worldwide, with the highest prevalence seen in the United States, with Denmark and Switzerland following close behind. The causes appear to be many, from low socioeconomic status and biomechanical strain to poor diet and psychosocial stress. In the U.S., spending on low back pain exceeds that of hundreds of other health conditions (including diabetes), with an estimated $134.5 billion dollars devoted to the condition in 2016.
Read More: Getting Back Pain While Working From Home? An Ergonomics Expert Offers Advice
Similar to a century ago, today’s evolutionary biologists continue to puzzle over human upright posture. Italian evolutionist, Telmo Pievani tells us that “the transition to bipedalism generated negative consequences in almost every part of the body.” Of course, one might reasonably wonder why, evolutionarily speaking, such an imperfection would be passed down from generation to generation. Wouldn’t natural selection weed out this kind of physical weakness?
According to Harvard paleoanthropologist Daniel Lieberman, conditions of poor posture, back pain, and obesity belong to a group of diseases which he calls “mismatch diseases,” maladies that arise due to novel environmental conditions for which the human body is poorly adapted. Lieberman, similar to evolutionists before him, blame industrialization for back pain. He contends that “from the body’s perspective, many developed nations have recently made too much progress. For the first time in human history,” he continues, “a larger number of people face excesses rather than shortages of food. Two out of three Americans are overweight or obese.” Obesity is not the only concern. “Depending on where you live and what you do,” Lieberman warns in his book, The Story of the Human Body, “your chances of getting low back pain are between 60–90 percent.”
In order to solve this (evolutionarily speaking) new problem of industrialized peoples, certain therapeutic body workers and self-designated ethnophysiologists have looked to indigenous populations who exhibit “primal posture.” One of the most prominent North American adherents to this approach is Esther Gokhale. Raised in India by European parents and later educated at Harvard and Princeton in biochemistry, Gokhale today is known as the “posture guru” of Silicon Valley, where she treats corporate heads of Google, Facebook, and other prominent online personalities, such as conservative journalist Matt Drudge. Gokhale developed an interest in human posture at a young age. With a tendency to exoticize, Gokhale recalls of her childhood in India, “I remember listening to my Dutch mother marvel at how gracefully our Indian maid went about her duties and how easily the laborers in the street carried their burdens.” Later in life, she documented the spinal health of indigenous peoples in Burkina Faso and Ecuador, photographing potters, basket makers, weavers, and head-carriers whom she admired for their ideal postures. Thereafter, she undertook training with Noëlle Perez, founder of the Aplomb method in Paris and one of the first Europeans to study under the Indian yoga master, B.K.S. Iyengar.
Largely devoid (at least at the outset) of breathing and meditative practices, Iyengar developed arguably the most biomedically friendly systems of yoga to come out of modern India, especially with its emphasis on biomechanical alignment and symmetry. When Perez opened her own Iyengar-inspired studio in Paris in the 1970s, she undertook doctoral studies in ethnophysiology at the École des Hautes Études en Sciences Sociales and researched nonindustrialized peoples of sub-Saharan Africa, where she claimed to have found bodies in what she called natural “aplomb.” Gokhale followed in Perez’s footsteps, and today contends that “most known risk factors [for back pain] can be mitigated by good posture.”
Gokhale’s insistence on the virtues of paleo posture align well with the 21st-century fitness industry, an enterprise known for creating slogans such as “sitting is the new smoking” and encouraging products that promote “primitive” eating and living. As in the early years of the poor posture epidemic, the evolutionary approach to understanding human posture—and now, by extension, low back pain—is good for the commercial marketplace. According to market analysts, posture correction technologies are expected to grow approximately 5.7 percent over the next five years, especially with rising demands due to the COVID-19 pandemic, with more at-home workers complaining of back pain.
On the face of it, posture improvement campaigns may seem rather innocuous. What is the harm, after all, of engaging in posture exercise programs? Of buying chairs, shoes, and devices that help to encourage it?
On an individual level, it is entirely possible that an enhanced sense of wellness can come from taking up yoga or purchasing an ergonomic chair. But when looking at the long history of posture improvement campaigns from an historical and structural standpoint, it becomes evident how value-laden they are, and how they can perpetuate sexism, ableism, and racism.
For example, scholars have, for some time, been aware of how, under the systems of slavery and colonialism, white men of science frequently assumed that Black and other non-white peoples could not feel pain, or if they did, it was felt less acutely compared to whites. Knowing this, one cannot help but wonder if the same bias has informed the work of today’s paleoanthropologists and ethnophysiologists, experts who observe so-called hunter-gatherers in Africa and deem such lifestyles to be pain free.
The social stakes of slouching are also higher for the politically marginalized. In recent years, researchers have found that, even today, prosecutors cite poor posture as a reason to deny African American men jury selection. In his autobiography about growing up in South Africa, comedian and political commentator Trevor Noah succinctly addresses the extra vigilance required of Black men and their posture in a white supremist society. “For centuries,” he writes, “colored people were told: Blacks are monkeys. Don’t swing from the trees like them. Learn to walk upright like the white man.”
Over the last century, health—and especially preventive health—has become increasingly commercialized: a product to be bought and sold, with the responsibility placed on individual consumers, making it a good that only those with a certain income can afford, rather than an ensured right for all. Those who cannot participate in the market are viewed as leading mismanaged lives, and when they sustain an injury that leads to permanent physical disability, are blamed for their condition. As long as posture surveillance is believed prevent low back pain, many posture and back health wellness programs are liable to create even greater health inequalities rather than mitigate them.
A recent study published by physical therapists working in Qatar, Australia, Ireland, and the United Kingdom speaks to the urgent need of the profession to dispel the medicalized myth that poor posture leads to bad health. “People come in different shapes and sizes,” they write, “with natural variation in spinal curvatures.”
In short, there is no single, correct posture. Nor does posture correction necessarily ensure future health. Maybe it’s ok to slouch from time to time, after all.
Excerpted from SLOUCH: POSTURE PANIC IN AMERICA © 2024 by Beth Linker. Reprinted by permission of Princeton University Press.
“}]]
Beth Linker explores how we became so obsessed with our posture—and the panic it has created.
Uncategorized, freelance
Health – TIME
Beth Linker explores how we became so obsessed with our posture—and the panic it has created.
Read more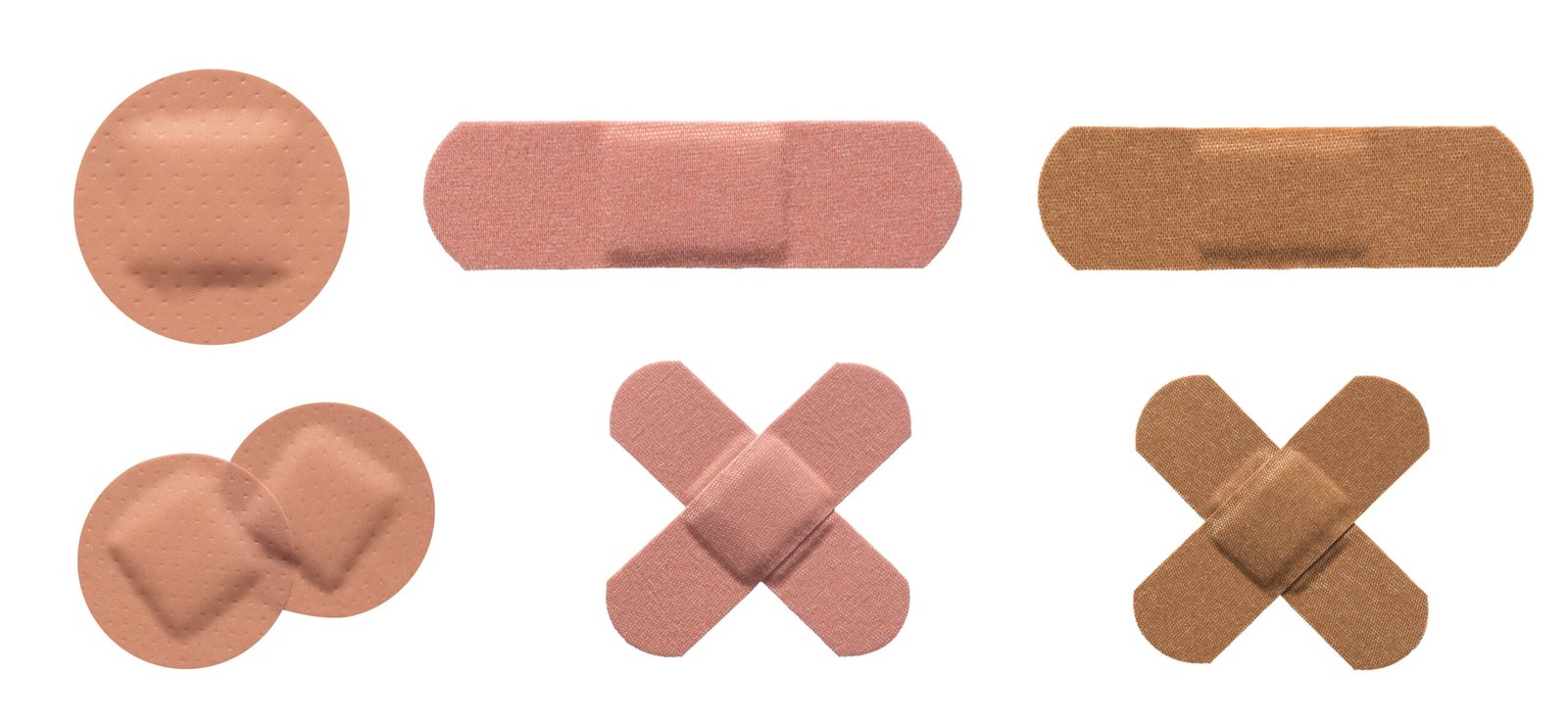
- Breaking News
- April 5, 2024
- 32 views
- 5 minutes Read
English News: Evidence of Dangerous ‘Forever Chemicals’ Found in Bandages
English News: Evidence of Dangerous ‘Forever Chemicals’ Found in Bandages
[[{“value”:”
Many brands of bandages may contain PFAS chemicals, according to a new report commissioned by Environmental Health News (EHN) and the consumer watchdog site Mamavation. Of the 40 bandages they analyzed in a lab, 65% contained signs of PFAS chemicals.
Also known as “forever chemicals,” because that’s approximately how long they linger in the environment, there are at least 12,000 types of PFAS. The health consequences of PFAS exposure are unclear. But this class of chemicals has been linked by the Environmental Protection Agency (EPA) to increased risk of certain cancers, decreased fertility, high blood pressure in pregnant people, developmental delays and low birthweight in children, hormonal disruption, high cholesterol, reduced effectiveness of the immune system, and more. According to the U.S. Centers for Disease Control and Prevention and the National Institute of Environmental Health Sciences, 97% of Americans have PFAS in their blood. The chemicals are found in thousands of common products, including food packaging, adhesives, carpeting, clothing, furniture, varnish, cleaning products, shampoo and cosmetics. They are also widespread in the water supply and food chain, and even in the rain.
[time-brightcove not-tgx=”true”]
Mamavation and EHN have made it something of a mission to conduct regular checks of various products, sending samples to laboratories to test them for the presence of organic fluorine, which is found in the presence of PFAS and is easier to detect than the chemicals themselves. A positive result for fluorine is considered a presumptive indicator that PFAS are there as well. In recent years, the two groups have made news with their discovery of PFAS-related chemicals in contact lenses, tampons and sanitary pads, dental floss, diapers, condoms, and sports bras.
Read More: Why Heart Disease Research Still Favors Men
To conduct the current analysis, the investigators selected 40 different bandage products from a variety of brands and sent them to a laboratory certified by the EPA. Bandages, of course, typically have two parts: the absorbent pad, which goes directly over the wound, and adhesive flaps. PFAS chemicals are sometimes added to the pads of bandages to help resist moisture, and to the flaps as an adhesive ingredient. Both were tested by the lab for fluorine levels at or exceeding 10 parts per million (ppm).
“Ten parts per million is the limit of detection, and that’s a large amount,” says Terrence Collins, professor of chemistry at Carnegie Mellon University and one of the scientists involved in the study. “We know that with endocrine disruption, there is no safe dose. They fiddle with hormonal control.”
Of the 40 bandages tested, 26 had fluorine levels ranging from 10 PPM to 374 PPM. Of 16 bandages manufactured in black or brown skin tones for people of color, 10 fell into that contamination range.
Products varied widely in the amount of fluorine they contained, even within the same overall brand. Bandages from CVS Health and BAND-AID, for example, fell into all three categories—those with the lowest, middle, and highest levels of fluorine—depending on the exact product tested.
Among the products that fared the worst were BAND-AID OURTONE Flexible Fabric BR65 Bandages, which weighed in at the peak of 374 PPM on the adhesive portion and 260 PPM on the absorbent pad. Bandages on the lower end of fluorine contamination included BAND-AID Water Block Tough Strips, at 13 PPM on the flaps and nothing detected on the pad; and CVS Gentle Fabric Hypoallergenic Bandages, with 10 PPM on the pad and fluorine-free flaps.
In an email to TIME, a spokesperson for CVS said, “We’re in the process of reviewing and evaluating the information in Mamavation’s bandage report.” Kenvue, makers of BAND-AID, did not immediately respond to a request for comment.
The bandages without evidence of PFAS tended to come from smaller brands, such as Patch Bamboo Bandages for Kids With Coconut Oil, with nothing detected on the pad or the flaps; and dark brown TRU COLOR Skin Tone Bandages, which also had no detectable fluorine.
Read More: Hormonal Birth Control Doesn’t Deserve Its Bad Reputation
While the pad, which makes direct contact with an open cut, would seem to present the greater contamination danger, mere contact with the skin via the adhesive flaps may be enough to allow PFAS to leach into the body, says Collins. “You have to assume that the body will have an affinity for a multitude of PFAS compounds.”
Bandages are just one possible route of exposure to PFAS. Our homes and personal care products are teeming with them. Though some PFAS may be excreted in urine and menstrual blood, once the chemicals get into the body, they can accumulate in the blood and tissues including the brain, liver, lung, bone, and kidney.
There’s not much consumers can do, and fixing the PFAS problem will not be easy. In February, the EPA tightened limits on nine varieties of PFAS that had previously been less regulated. Additionally, legislation is pending or has been passed in seven states—California, Colorado, Maryland, Washington, Rhode Island, Minnesota, and Connecticut—to limit or prohibit PFAS in a range of consumer products, as well as in firefighting foam. But they are already ubiquitous in the environment.
“Once you make them, you can’t just crack a whip and call them back,” says Collins. “The stuff that’s out there will accumulate in living things that die and get covered up with sediment. A few thousand years from now,” he predicts, “you’ll be able to dig back and find the fluorine layer.”
“}]]
A new report found evidence of PFAS in 65% of the bandages they analyzed.
Uncategorized, healthscienceclimate
Health – TIME
A new report found evidence of PFAS in 65% of the bandages they analyzed.
Read more
- Breaking News
- April 5, 2024
- 46 views
- 2 minutes Read
English News: COVID-19 ‘Radically’ Changed the Leading Causes of Death
English News: COVID-19 ‘Radically’ Changed the Leading Causes of Death
[[{“value”:”
COVID-19 became the second leading cause of death globally in the year after it was declared a pandemic, according to a study published in the Lancet.
While heart disease remained the top killer, COVID “radically altered” the main five causes of death for the first time in 30 years, displacing stroke, the publication said. In 2021, 94 in every 100,000 people died from COVID, on an age-standardized basis.
Since 1990, global life expectancy increased by 6.2 years, mainly due to reductions in death from diarrhea and lower respiratory infections and better outcomes for people suffering from a stroke or ischemic heart disease.
Read More: Ozempic Gets the Oprah Treatment in a New TV Special
“Our study presents a nuanced picture of the world’s health,” said Liane Ong, co-first author of the study and a lead research scientist at the Institute for Health Metrics and Evaluation. “On one hand, we see countries’ monumental achievements in preventing deaths from diarrhea and stroke. At the same time, we see how much the COVID-19 pandemic has set us back.”
From 2019 to 2021, progress was made in preventing deaths for most other top causes of death except for Alzheimer’s disease and other dementias and malaria.
The study is thought to be the first that compared deaths from COVID to deaths from other causes. It tracked 288 causes of death in 204 countries and territories and 811 subnational locations.
“}]]
COVID-19 became the second leading cause of death globally in the year after it was declared a pandemic.
Uncategorized, COVID-19, healthscienceclimate, wire
Health – TIME
COVID-19 became the second leading cause of death globally in the year after it was declared a pandemic.
Read more
- Breaking News
- April 5, 2024
- 49 views
- 3 minutes Read
English News: Is It Safe to Eat Eggs and Chicken During the Bird Flu Outbreak?
English News: Is It Safe to Eat Eggs and Chicken During the Bird Flu Outbreak?
[[{“value”:”
The ongoing outbreak of bird flu has infected at least one person in the U.S. and has raised questions about how safe poultry meat and eggs are to eat right now.
So far, there have been no reported cases of spread among people, or of a person contracting this strain of avian influenza (also known as H5N1) from contaminated egg or poultry products, according to the U.S. Centers for Disease Control and Prevention (CDC). The CDC says that the current public health risk is “low.”
[time-brightcove not-tgx=”true”]
Here’s what scientists know right now about bird flu and food safety.
Eggs
The largest producer of eggs in the country, Cal-Maine Foods in Texas, temporarily stopped production at one of its facilities on Apr. 2 after H5N1 was identified there. The company also culled more than 3% of its flock in response to the outbreak.
Eggs from infected chickens are unlikely to be on supermarket shelves, the FDA says. That’s because in the time that it takes to detect an avian flu virus in a flock of egg-laying chickens, 99.99% of eggs would not have reached store shelves yet, since they would still be in the process of being distributed. That prediction comes from a model for estimating the risk of human exposure from avian flu outbreaks that was developed by the U.S. Department of Agriculture (USDA) and the U.S. Food and Drug Administration (FDA) in 2010. According to that assessment, even if an infection among chickens was discovered after eggs had hit supermarket shelves, more than 98% of potentially contaminated eggs could be removed from stores after a recall was issued.
Read More: Is Eating a Plant-Based Diet Better For You?
Another safeguard: pasteurization inactivates viruses in eggs and therefore eliminates most risk to human health. Properly handling eggs—including avoiding cross contamination of any raw products with other foods—and cooking them at least until the yolks and whites are firm will further reduce any risk of infection.
Poultry meat
Like it is with eggs, the risk of buying infected chicken at the grocery store is very low, according to the USDA and FDA. The model predicted a 95% probability that infected poultry would not make it to stores, since the virus would lead to relatively high mortality among the chickens, and farmers would be aware of the infection before the poultry was prepared for sale. However, the scientists determined that there is a 5% chance that infected chickens reaching market size would be slaughtered and sold before the virus was detected.
Read More: Why Your Diet Needs More Fermented Pickles
The best way to prevent that from happening is to increase testing of flocks on farms, the risk assessment concluded. Farmers can also detect illness in their flocks by monitoring how much feed the birds eat, since birds tend to eat less when they’re sick. According to the risk assessment, keeping track of feed consumption can lead to a 96% chance that an infected chicken is not processed for market, and can reduce the risk of human disease by 23 fold, while checking for signs of sickness leads to a 95.5% chance that infected chickens are not processed for market and reduces the risk of human illness by 8-fold.
As an added safety measure, keep raw chicken away from uncooked foods and cook chicken to 165°F, which likely inactivates any virus that could make people sick.
“}]]
Experts say the risk is low, but taking these precautions is a good idea.
Uncategorized, healthscienceclimate
Health – TIME
Experts say the risk is low, but taking these precautions is a good idea.
Read more
- Breaking News
- April 5, 2024
- 58 views
- 11 minutes Read
English News: Why Heart Disease Research Still Favors Men
English News: Why Heart Disease Research Still Favors Men
[[{“value”:”
Published in partnership with The Fuller Project, a nonprofit newsroom dedicated to the coverage of women’s issues around the world.
Katherine Fitzgerald had just arrived at the party. Before she could even get a drink, she threw up and broke out in a sweat. “I was dizzy. I couldn’t breathe. I had heart pain,” Fitzgerald says.
She knew she was having a heart attack.
[time-brightcove not-tgx=”true”]
What she didn’t know then was that the heart attack could have been prevented. Fitzgerald, a health-conscious, exercise-loving lawyer, should have been taking statin drugs to stop the buildup of plaque in her arteries that caused the heart attack and two others that followed.
Fitzgerald’s case illustrates a dangerous gap in medical care between men and women. While they are equally likely to suffer heart attacks, women are more likely to die from theirs. It’s one of the many symptoms of the medical system’s neglect of women.
Life-saving statins, like so many other medications, have been developed based on clinical trials that primarily recruited men. As a result, many women like Fitzgerald don’t receive prescriptions for the drugs that could help them the most, says Dr. Laxmi Mehta, director of Preventative Cardiology and Women’s Cardiovascular Health at The Ohio State University.
“There were a lot of trials. But women weren’t included as much,” says Mehta, who serves on the American Heart Association’s Research Goes Red Science Advisory Group. When women need treatment for heart conditions, she says, “we are assuming we are providing the best care based on data from men.”
Read More: What It Means if You Have Borderline High Cholesterol—And What to Do About It
More than 30 years ago, Congress directed the National Institutes of Health to include as many women as men in clinical trials. But while some progress has been made, equity remains elusive. And that’s dangerous for women. “Since 2000, women in the United States have reported total adverse events from approved medicines 52% more frequently than men, and serious or fatal events 36% more frequently,” research firm McKinsey & Company said in a report released in January.
Now, the Biden administration is taking a run at it.
Last year, the administration established a White House Initiative on Women’s Health Research and, in February, it announced it would be dedicating $100 million to the newly formed Advanced Research Projects Agency for Health (ARPA-H) to spearhead efforts to increase early stage research focusing on women.
“For far too long, scientific and biomedical research excluded women and undervalued the study of women’s health. The resulting research gaps mean that we know far too little about women’s health across women’s lifespans, and those gaps are even more prominent for women of color, older women, and women with disabilities,” Biden said in an executive order signed in March.
Heart disease should be a bright spot in this black hole of medical research. It was the recognition in the 1980s that heart disease was killing women at similar rates to men that kickstarted passage of the 1993 law requiring equity in clinical trials. The American Heart Association has spent decades funding research and leading awareness campaigns about women’s risks.
But gaps persist, says Dr. Martha Gulati, president of the American Society for Preventive Cardiology and a cardiologist at Cedars-Sinai Hospital in Los Angeles. “We don’t get represented in trials,” Gulati told a seminar sponsored by the Society for Women’s Health Research in February.
Read More: Why Are So Many Young People Getting Cancer?
One example: Dr. Safi Khan of West Virginia University and colleagues reviewed 60 trials of cholesterol-lowering drugs conducted between 1990 and 2018. Not even a third of the people enrolled—28.5%—were women, they reported in JAMA Network Open in 2020. The trials’ findings likely did not accurately represent the public as a whole, they say.
“Medical research is several steps behind on women and heart disease, and that is a major contributor to ongoing ignorance about the problem on the part of both the public and a range of medical professionals,” says Dr. Harmony Reynolds, a cardiologist at NYU Langone Health. “Everywhere along the way, there is different treatment for women, and there is some bias there.”
Statins have been widely described as wonder drugs, lowering the risk of major heart events such as heart attack or stroke by about 25%. Women are less likely than men to be offered these drugs. And when they do take them, women are more likely to stop using them because of perceived side effects. But no major study digs into the actual rate of side effects among females, or what might lie behind such differences.
Further studies might uncover additional benefits, says Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. There are hints that statins might lower a woman’s risk of dying from cancer, including ovarian cancer.
Failure of recognition
Fitzgerald was 60, had higher-than-optimal blood pressure, unhealthy cholesterol levels, and a family history of heart disease, says Reynolds, Fitzgerald’s new cardiologist. “Katherine had multiple risk factors. Many of my patients are told their blood pressure and cholesterol are ‘borderline’ when really they should be treated,” she says.
Doctors often blame women for failing to recognize their own heart disease symptoms, but the evidence shows medical professionals miss them, too.
The symptoms of heart attacks in men are widely known: crushing chest pain, a telling sensation in the left arm, or sudden collapse. Women, on the other hand, often feel nausea, jaw pain, or lightheadedness,
Fitzgerald did recognize her symptoms. At the party where she suffered her first heart attack, she begged for an ambulance. But other guests, including a physician friend, said they didn’t think she needed medical attention.
When paramedics finally arrived, they, too, dismissed her fears and diagnosed a panic attack. They sent her home. “If I had been a man, there is no way the paramedic wouldn’t have taken me to the hospital and I wouldn’t be in the mess I am now,” Fitzgerald says.
Fitzgerald waited two days to visit an emergency room. By then, some of her heart muscle had died. She received two stents to hold open clogged arteries, but suffered two more heart attacks in the following months. She now stays out of the courtroom and sticks to less-stressful desk work.
“I take care of all these young women with heart attacks and I hear so many stories about people saying they were ignored,” says Reynolds.
Waiting for attention
The problem is not just anecdotal. Reynolds and colleagues studied the problem by looking at more than 29 million emergency room visits by people under 55 reporting chest pain.
“In that study we show young women coming in with chest pains and they are waiting longer to be seen,” Reynolds says. “The women are waiting too long and women of color were waiting even longer. So we know there is some subtle bias there.”
Read More: What the Science Says About the Health Benefits of Vitamins and Supplements
Doctors can use risk calculators to try to forecast a patient’s future likelihood of heart disease and treat accordingly. But Dr. Stephanie Faubion, medical director of the Menopause Society, says they do not work well for women.
“That is because we are still using those that were developed and made for men,” says Faubion, who is also director of the Mayo Clinic Center for Women’s Health in Jacksonville, Florida.
Women have many specific heart risks. They have smaller coronary arteries, thinner heart walls, and suffer more heart damage from diabetes. Pregnancy can raise risks in various ways. Autoimmune diseases such as rheumatoid arthritis also add heart disease risks, and women are far more likely than men to have these conditions.
Women who start menstruation early, or who reach menopause early, have higher heart disease rates. Birth control pills can raise the risk for blood clots, strokes, and heart attacks.
Perhaps the most recent instance of women being left out of heart disease research can be seen in the trials of highly popular diabetes drugs such as semaglutide, sold under the brand names Ozempic and Wegovy.
The drugs cause dramatic weight loss, which made researchers wonder if they might lower heart disease rates, too. They do, according to several studies, and the U.S. Food and Drug Administration now approves their use to prevent heart disease.
But none of the weight-loss trials, published in prestigious medical journals such as the New England Journal of Medicine and the Journal of the American Medical Association, break out separate data on men and women. And while the weight-loss studies did include far more women than men, many of the follow-on heart disease trials did not.
“They report the sex. They report ‘we have this many men, this many women,’” says Faubion. “They didn’t disaggregate the data on sex so they don’t know if it works better, the same, or worse in women than it did in men.”
Left out
Dr. Robert Kushner, a professor of medicine at Northwestern University who led some of the weight-loss studies, says he was surprised at the discrepancy between the enrollment of women in the obesity trials of semaglutide—in which about three-quarters of volunteers were women—and in the heart disease trials, in which women represented fewer than 28% of participants.
He says researchers recruited people already being treated for heart disease. “Predominantly, the ones who are getting care and being seen around the world were men,” Kushner says.
Kushner says he has yet to analyze results in his trial of semaglutide and weight loss by sex.
Missing out on breakthroughs
Harvard Medical School’s Manson has been sounding the alarm on discrepancies in medical research for decades.
“Raising more questions is what leads to the major breakthroughs,” she says.
Yet she has been mostly ignored, even though she helped lead the largest-ever study looking specifically at women’s health—the Women’s Health Initiative, which involved more than 160,000 women over 15 years.
The study was initially designed to see if hormone therapy in women past menopause could reduce their rising rates of heart disease and breast cancer. It also later looked for evidence of effects on bone strength, other cancers, dementia and quality of life.
The first results were startling. The hormone therapy used in the trial raised the risk of breast cancer and failed to reduce heart disease.
Read More: Menopause Is Finally Going Mainstream
“Many clinicians stopped prescribing hormone therapy altogether. Many women tossed their pills and patches,” Manson says. When the trial started, an estimated 40% of menopausal women used hormone therapy. Now, Manson estimates, only about 4% do.
The study has since been shown to have been flawed. The average age of the women in the study was 63—well past menopause. And the hormone therapy used was a high-dose hormone distilled from horse estrogens.
Later studies have indicated that lower doses and different formulations such as patches, given to women as they start menopause, may be much less harmful while reducing hot flashes, sleep loss and other symptoms. “These formulations don’t go to the liver and should be safer,” Manson says. There’s also tantalizing evidence they may lower the risk of heart disease.
Meanwhile, the lack of data means that many women who would benefit from hormone therapy are not getting it, says Faubion.
Back in 1993, it took the considerable efforts of Dr. Bernadine Healy, the first female director of the NIH, to persuade Congress to directly fund medical research on women and heart disease.
“They are just not going to do that again. It’s too expensive,” says Faubion.
Biden asked Congress for $12 billion to improve research planning and to set up a network of research centers to focus on women’s health. And NIH has encouraged requests for money to study women in particular.
But when Congress passed a last-minute spending bill in March, it kept health funding flat. The Republican-led House did not address Biden’s request or allocate any cash for additional research into women’s health.
Sign up for the Fuller Project’s newsletter, and follow the organization on X or LinkedIn.
“}]]
Life-saving statins, like so many other medications, have been developed based on clinical trials primarily made up of men.
Uncategorized, freelance, healthscienceclimate
Health – TIME
Life-saving statins, like so many other medications, have been developed based on clinical trials primarily made up of men.
Read more
- Breaking News
- April 4, 2024
- 28 views
- 2 minutes Read
English News: Scientists Find New Genetic Variants for Obesity
English News: Scientists Find New Genetic Variants for Obesity
[[{“value”:”
Researchers believe they have discovered a new biological mechanism for obesity, pointing to rare variants on two genes that dramatically increase the risk of carrying excess weight.
Research published in the journal Nature Genetics on Thursday points to variants that raise the chance of being obese by as much as six times. Unlike other known variants that affect weight gain in children, these only appear to play a role in adults.
[time-brightcove not-tgx=”true”]
Unraveling obesity’s mechanisms could help scientists develop new drugs, or tailor existing ones, for a condition that now affects one in eight people. For the first time, patients can now take highly effective medicines to shed unwanted weight. The revolution, led by drugmakers Novo Nordisk A/S and Eli Lilly & Co., carved open a market that could surpass $100 billion globally by 2030.
Read More: Ozempic Gets the Oprah Treatment in a New TV Special
Using data from over 500,000 people, scientists from the Medical Research Council at the University of Cambridge found variants in two genes called BSN and APBA1 that increased the risk of obesity in adults.
The variants in BSN, also known as Bassoon, were associated with an increased risk of diabetes and fatty liver disease. The Bassoon variants affect about 1 in 6,500 adults, the researchers said.
The hypothesis is that as people who have these gene variants get older, neurons in their brain start to degenerate, removing “some of the key circuits within the brain controlling food intake and therefore you end up with obesity,” said Giles Yeo, one of the authors of the study and a professor at the MRC Metabolic Diseases Unit.
The Bassoon variant may one day help drugmakers develop preventive medicines, according to Yeo. The question would be, “can we actually slow down the process, prevent the process from happening to begin with, so that then we prevent more people from ending up with obesity, particularly in adulthood.”
The researchers used the UK Biobank database and worked with AstraZeneca Plc to check that their findings applied beyond people of European ancestry, using data from Pakistan and Mexico.
Astra is one of the latest drugmakers to join the obesity race, having clinched a deal last year to buy an experimental pill that’s still in early-stage tests.
“}]]
Rare variants on two genes dramatically increase the risk of carrying excess weight.
Uncategorized, healthscienceclimate, wire
Health – TIME
Rare variants on two genes dramatically increase the risk of carrying excess weight.
Read more
- Breaking News
- April 4, 2024
- 45 views
- 9 minutes Read
English News: How to Talk to Kids When a Parent Has Cancer
English News: How to Talk to Kids When a Parent Has Cancer
[[{“value”:”
The U.S. is expected to hit a bleak milestone this year: For the first time, more than 2 million people will be diagnosed with cancer. More than 600,000 will die, according to projections from the American Cancer Society.
Yet when you consider how many people are affected by a single diagnosis, those numbers balloon. As people with cancer grapple with fears about their health, they often describe being equally anxious about how their news will affect their family. When Catherine, Princess of Wales, revealed on March 22 that she was being treated for cancer, she emphasized that she and her husband had “taken time to explain everything” to their three young children “in a way that is appropriate for them.”
[time-brightcove not-tgx=”true”]
Whatever your treatment might entail, it’s helpful to know how to discuss your prognosis with your loved ones so you can prepare them for the road ahead, as variable and unknown as the future may be. That’s especially true with children, who are often more intuitive than you may realize.
“Kids are incredibly perceptive on picking up that something is off,” says Dr. Amishi Y. Shah, a genitourinary medical oncologist and associate professor at the University of Texas MD Anderson Cancer Center in Houston. “In general, being transparent about what’s going on with kids is a good policy.”
Of course, each family will talk about a cancer diagnosis with children differently. “There’s not necessarily a one-size-fits-all [approach],” says Amanda L. Thompson, chief of pediatric psychology and director of pediatric programs at Life with Cancer, a northern Virginia nonprofit providing support and education for people affected by cancer. “What you’re going to disclose is going to depend on the age of your child, their maturity, their own experience with or exposure to illness within the family or close friends, and more.”
Here, cancer experts and mental health professionals share tips for approaching this conversation with care and compassion.
Read More: Kate Middleton Had to Tell Her Kids About Her Cancer Diagnosis. These Parents Know What That’s Like
Plan ahead
This probably isn’t the best time for an off-the-cuff, improvised conversation, notes Shannon Coon, children’s program coordinator at the cancer support organization CancerCare. “Write down what you want to say before the conversation happens, and practice prior,” she says. That might make it easier to speak in a calm and reassuring voice when the time comes, she says.
Think about who you might want to have with you, as well, Coon adds: Do you want to speak with your children individually? Do you want your partner to be there? Should any other adults in their lives be present?
Create a welcoming environment for the conversation
Choose a calm, safe space and time to bring up your diagnosis with childrens. Make sure you have plenty of time to answer questions without having to rush off to another part of your day, says Thompson.
Picking your moment counts in other ways too. It might help to identify when your family already comes together in a way that feels “connected, comfortable, and normal,” says Max McMahon, a licensed independent clinical social worker at the Lank Center for Genitourinary Oncology at Dana-Farber Cancer Institute in Boston. “Is the dinner table when good conversations happen? Is it when you go out for bagels on Saturday mornings? When do your kids seem to want to talk about things or process their day?” he asks.
Whatever the setting, your goal should be to welcome discussion. “We’re creating an environment where it’s OK to talk about the hard things out in the open,” Thompson says.
Stick to age-appropriate terminology
Tailor the language you use based on the age of the child you’re talking to. For a young child, that might look like: “‘Mommy is sick. She has something called cancer. The doctors are doing everything in their power,’” Coon says. You might even point to the sides of your back and explain the cancer is in your kidneys.
Older children will be able to understand more, so the conversation may be more detailed, but they’re also in a different emotional space. “I’ve found the most difficult [scenario] is when the kids are teenagers,” says Dr. Toni K. Choueiri, director of the Lank Center. “They’re going through a lot of changes, and now you add to it.”
Use concrete language
It can be tempting to gloss over unnerving topics, but using the word “cancer” can actually help defuse the situation, Thompson says. “Harry Potter said ‘Voldemort.’ He gave the big bad villain his name to take away some of his power. We have to use that word matter-of-factly. It is important for children to know it’s something they’re going to hear.”
Similarly, it’s helpful for children to hear clear language about death, “even though it is incredibly difficult … especially if you’re the parent who is ill and facing your own mortality,” she adds.
That doesn’t mean you have to state simply, “I’m dying,” McMahon says. You might say something like, “This is a serious, advanced disease, and I’m getting treatment for it, [but] this disease can’t be cured, and I will die from it,’” he says.
Using euphemisms or otherwise prettifying language can lead to children interpreting things too literally. “Sometimes children think ‘heaven’ is a place they can visit,” Coon says, or that they can go find a loved one who has been “lost,” Thompson adds.
Discuss visible physical changes
Immunotherapy and targeted drug therapy for cancer can cause side effects like joint and abdominal pain, diarrhea, loss of appetite, and fatigue, all of which children might notice. And if they do, it’s better to be upfront about it. “Otherwise, they’re wondering in silence,” McMahon says.
Some changes will be more obvious than others. For example, Choueiri says, if you’re dealing with diarrhea and your home has only one bathroom, it would be nearly impossible to hide the fact that you’re using it every hour.
But even if side-effects are more nuanced—maybe you’re walking more tenderly because you’re in pain, or you’re losing weight because you’re not hungry—embrace opportunities to explain where you can. You might try: “‘Dad is in pain. Do you want to know what’s happening inside Dad’s body?’” McMahon advises. Some parents worry this will create more anxiety for a child, “but kids often have anxiety about what they don’t know, so information is helpful for most children.”
Read More: Kate Middleton Is Receiving Preventative Chemotherapy. Here’s What That Is
Explain how their lives may change
Consistency generally makes children feel secure, and cancer can certainly disrupt your schedule. Aim to explain to children what you expect to shift in your routine. “They’re going to want to know, ‘What does this mean for my family and what we do? Does this mean someone else picks me up from school? Are we still going on the trip we take every year?’” Shah says.
Reassure kids that even if someone else will handle school pick-up, their needs will be met and they’ll still be cared for and loved. Consider sharing your treatment calendar with older children, so they can anticipate some of those changes on a weekly or monthly basis.
Answer questions honestly
After you’ve disclosed your diagnosis for the first time, lean on a child’s curiosity to shape your ongoing conversations. Answer questions as they come up, then pause for a moment to see what other questions arise (if any). Kids will likely come up with questions about a parent’s cancer that you don’t know the answers to. “The reality is, we probably won’t have all the answers. Often our physicians don’t even have all the answers,” Thompson says.
In those cases, it’s OK to tell a child you don’t know. “Let them know that when you do know, you’ll get back to them as soon as possible,” Coon says. You can show them you mean it by keeping a running list of unanswered questions and bringing it to your next visit with your oncologist.
Check in
Just as you’ll need more than one visit with your oncologist over the course of treatment, you’ll likely need more than one conversation with a child to fully discuss their feelings about your prognosis. Touch base with specific questions that welcome their curiosity rather than broad questions like asking how they’re doing, suggests the American Cancer Society. You might start with a question like, “‘What changes have you noticed with Dad lately?’” Choueiri suggests, or “‘You’ve noticed Mom has had to go to the hospital more. Do you have any questions about that?’” McMahon says.
Older children can take even more ownership in shaping these conversations. “I often recommend asking how they want to be updated along the way,” Thompson says. “Do they want to know the details? Do they want to talk about it in the morning or the evening? What would be most helpful for them?”
Lean on the services meant to help
Your medical team can likely connect you with support services at your treatment center to assist you in navigating these difficult conversations. You might have oncology social workers, nurse navigators, and other experienced staff members available to you and your children. “It’s our job to guide you to the resources that can help. You don’t have to do it alone,” Shah says.
That’s especially true if children start exhibiting any signs that they need more support than you’re equipped to give them, such as experiencing changes in sleeping or eating patterns, social withdrawal, fighting with their siblings or friends more often, or more frequent bedwetting.
Organizations like the American Cancer Society have information and support groups for parents and caregivers. Nonprofits like CancerCare offer children’s programs free of charge. And there are even Facebook groups for people with specific types of cancer where you can find comfort in knowing you’re not alone.
Talking about a parent’s cancer with children is never easy, but it’s helpful for your kids and your relationship. “In general, know it’s going to be difficult and emotional in the moment,” Coon says, “but it’s so important to have open and honest conversations throughout the cancer journey.”
“}]]
It can help to choose your words wisely—but you don’t have to shy away from heavy conversations.
Uncategorized, Evergreen, freelance, healthscienceclimate
Health – TIME
It can help to choose your words wisely—but you don’t have to shy away from heavy conversations.
Read more
- Breaking News
- April 4, 2024
- 48 views
- 6 minutes Read
English News: Your Doctor’s Words Could Make You Sick
English News: Your Doctor’s Words Could Make You Sick
[[{“value”:”
“You may feel a sharp pinch, but it will all be over quickly.”
Before the COVID-19 jab was plunged into our arms, most of us probably heard words similar to these. After the anticipated pinch, the nurse or doctor likely told us something about possible vaccine side effects. For one of us, the nurse’s forewarning was rather specific: “Around 12 hours from now you may experience a pain in your arm or feel flu symptoms. But don’t worry,” the nurse aimed to reassure. “This can be easily managed by Tylenol.”
[time-brightcove not-tgx=”true”]
Sure enough, like clockwork, 12 hours later, the symptoms manifested.
An estimated 30% of people who received the COVID-19 vaccine also reported nasty side effects. Making matters worse, like a nightmarish self-fulfilling prophecy, the very words used by clinicians might well have caused some of this harm. Of course, doctors and nurses do not deliberately set out to hurt patients—far from it. They want to ensure that patients are fully informed. However, as our research shows, their words might unintentionally ramp up the effects of a psychological phenomenon that operates under the radar. This phenomenon is called the “nocebo effect.”
Characterized as the “evil-twin” of the placebo effect, nocebo effects are harms that arise from negative expectations. While placebo effects are those beneficial outcomes that arise when we expect to feel better and, as a result, do, nocebo effects are what happen when we expect to feel worse.
Read More: The Placebo Effect Is Real, and Scientists May Be Able To Predict Who Responds
Today, we expect our doctors to give information to us straight. Gone are the days when doctors could wilfully withhold information from patients, even if they believed doing so would make patients feel better. Yet, the best-known phrase from medicine’s oldest creed, the Hippocratic Oath, is “First, do no harm.” Nocebo effects are one of medicine’s natural disruptors: they present a challenging scenario because, sometimes, information may be bad for our health. Balancing honesty against the risks of harm is no easy feat and is one area where medical ethicists, health researchers, patients, and clinicians need to put their heads together.
COVID-19 offered an unprecedented global experiment into the size and significance of this effect. In 2022, placebo researcher Julia Haas led a review of COVID vaccine clinical trial data and concluded that the nocebo phenomenon could account for as much as three quarters of the side effects associated with the jabs. The evidence for this startling finding comes by comparing side effects between patients allocated to the placebo shot versus those allocated to the real shot in the vaccine trials. Those receiving only a saline injection with no effect on the body still reported many unwanted side effects. It is possible that some of these effects might have been due to “symptom misattribution.” At any given time, some of us may experience low grade aches and pains, such as headaches, or fatigue, and knowledge that the vaccine causes these effects might draw our attention to symptoms we’re already experiencing. Alternatively, some negative symptoms might have been caused, or worsened, by nocebo effects.
Beyond COVID-19, a growing body of research shows that nocebo effects may be commonplace in medicine and that the verbal suggestions uttered by clinicians really do matter. In one experimental study in 2004, radiology professor Dr. Elvira Lang and her colleagues found that warning or even sympathizing with patients about painful or undesirable experiences following an intervention increased pain and anxiety. In another 2003 study of beta-blockers for cardiac disease and hypertension, telling patients that treatment side effects might include erectile dysfunction (ED) led to a doubling of patients reporting this problem compared with those not given information about ED risk.
In 2010, Dr. Dirk Varelmann, a specialist in anesthesia and pain management at Beth Israel Deaconess Medical Center in Boston, wanted to explore whether the way in which a local anesthetic injection was described to patients would influence pain. Varelmann led a study where one group was told, “You will feel a big bee sting; this is the worst part;” the other group was informed, “We are going to give you a local anesthetic that will numb the area, and you will be comfortable during the procedure.” Those who were told they would feel a sting—that is, the patients receiving a negative suggestion—reported significantly more pain after the injection even though both groups got the same anesthetic. Varelmann’s conclusion was that, “using gentler, more reassuring words” could improve patients’ experience during invasive medical procedures.
Studies like this expose the ethical dilemma that nocebo effects invite. Since April 2021, patients in the U.S. have had the right to read their online medical records. Access rights include test results, medication lists, and the very words written by clinicians. Patients appreciate this. Surveys in the U.S. and other countries where access has been rolled out reveal patients who read their electronic medical records feel more in control of their care, and report better understanding and recall about their treatment plans. People who poke their noses into their records also report better understanding of the side effects of the medications they are prescribed.
However, there is a catch. In a study one of us conducted in 2021, some enlightened patients said they worried more about their medications after reading their clinical records. And while the connection has only been hypothesized, we shouldn’t be surprised if the language doctors use in our records gives nocebo effects unfettered free reign. In fact, as many as half of all patients in the U.S. who are prescribed medications for chronic conditions fail to take their meds leading to an estimated 100,000 preventable deaths and $100 billion in costs every year. Side effects are one of the main reasons patients discontinue treatments. If we can solve the nocebo problem, we might do a better job of keeping more people on their medications and staying healthy.
Nocebo effects are relevant even beyond the doctor’s office. They invite challenging questions about how governments should frame public health information, and how advertisers ought to sell their drugs on TV. The free press is a pillar of democratic societies, but even here the nocebo phenomenon raises interesting novel concerns. If journalists reporting on health veer into sensationalism and scaremongering, and this literally causes readers harm, was their choice of words unethical?
This brings us back to coronavirus. An estimated 70% of the world’s population received at least one COVID-19 jab. But many skipped their second shot, some because of fears about the vaccine’s side effects. Perhaps not even the most ardent conspiracy theorist could have imagined that a humble mind-body effect might have played a role in the pandemic’s gloomy story. But they should think again.
Knowledge is power, but it’s as equally important to remember that words matter. Let us not delay the “nocebo” conversation any longer.
“}]]
Words can make you sick, a phenomenon known as the nocebo effect. This poses an ethical problem for our health system.
Uncategorized, freelance, History
Health – TIME
Words can make you sick, a phenomenon known as the nocebo effect. This poses an ethical problem for our health system.
Read more
- Breaking News
- April 4, 2024
- 51 views
- 7 minutes Read
English News: The Menstrual Mood Disorder You’ve Never Heard About
English News: The Menstrual Mood Disorder You’ve Never Heard About
[[{“value”:”
Ever since she was a teenager, Tanya knew her mood swings were a problem. She had periodic bouts of anger and depression that left her wanting to die. Her life was a roller coaster of highs and lows but doctors couldn’t figure out what was wrong. Five years ago, she decided she’d had enough. She wanted to end her life.
Tanya managed to talk herself out of it and instead did some googling. She stumbled across a website about premenstrual dysphoric disorder (PMDD), a menstrual mood disorder, that impacts roughly 3 to 8% of menstruators. PMDD means having severe and debilitating mood swings right around one’s period. Around a third of people with PMDD have attempted suicide, and over 70% have regular suicidal ideation.
[time-brightcove not-tgx=”true”]
“It just hit me,” Tanya told me. “I went through my life and so many moments made sense.” She called her doctor the next day. He sent her to get tested for diabetes.
Tanya finally managed to get a PMDD diagnosis in 2019 at the age of 26, but she was haunted by the question: Why had she never heard of PMDD before and why was it so hard to get a diagnosis?
Although research shows suicidal ideation is linked to specific times during the menstrual cycle, today most people still haven’t heard of PMDD, including doctors. According to a 2022 survey of PMDD patients, over a third said their general practitioners had no knowledge of premenstrual disorders, and about 40% said their mental-health-care providers had no knowledge of premenstrual disorders. But PMDD has been around since periods have been around and we’ve known about it for nearly a century.
So why aren’t we getting people the help they need? The answer, as history shows, is more complicated than we think.
While the menstrual cycle has been notoriously understudied, the first papers on PMDD appeared in 1930s. In the 1950s British physician Dr. Katrina Dalton began studying PMDD—or “premenstrual syndrome” as she called it, and opened a clinic in London. Still, PMDD mostly flew under the radar until 1980, when Dalton served as a medical expert for three women accused of crime. During the trials Dalton showed that the women committed the crimes right before their period, and that their symptoms disappeared with treatment. She was able to get them a reduced sentence.
Overnight there was a media boom around PMS. The magazine Glamour even polled readers about the validity of using PMS as a legal defense: (24% were for, 71% against, and 5% unsure). As a result, the growing awareness around PMS bled over to the medical community. In 1984 psychiatrist Robert Spitzer proposed PMS should be added to the Diagnostic and Statistical Manual of Mental Disorders (DSM), the handbook used by doctors to diagnosis mental health problems. Spitzer was the chair of the committee revising the third version of the DSM, and he’d been getting several invites to conferences about PMS. Adding PMS to the DSM meant that the medical community was recognizing it as a formal disorder that could be diagnosed and treated.
Read More: 5 Foods That Ease PMS Symptoms
However, experts were divided on where to draw the line between PMDD (the severe, debilitating mood swings) and PMS (garden variety grumpiness and irritability). When the Washington Post asked experts about the prevalence of PMS in 1984, estimates ranged from 3% to 90% of women. In a sense, both of these estimates were true: only a few people have severe symptoms, but up to 90% of people do have mild symptoms before their period. It became clear that experts were conflating PMDD and PMS and this was reflected in popular culture. Suddenly, anyone who had a period was seen as unstable. Products with sexist jokes abounded, such as greeting cards that read “What’s the difference between a woman with PMS and a terrorist? Answer: You can negotiate with a terrorist.”
Controversy erupted. A group of feminists spearheaded a campaign to stop PMDD’s inclusion in the DSM. They argued that including PMDD would be tantamount to calling menstruation a mental illness. Much of their reaction was rooted in the atmosphere of the ‘70s and ‘80s as women were fighting for gender equality on several fronts from work to reproductive rights. In the 1970s, for the first time, over half of women were working outside the home. Congress passed Roe v. Wade protecting the right to abortion. However, this equality was also precarious and under threat—conservatives defeated the Equal Rights Amendment which would have prohibited gender discrimination. For feminists, PMDD and the sexist jokes it generated seemed to be another attempt to discredit women and chip away at the progress feminists had made for women’s rights.
One of PMDD’s major critics, Dr. Joan Chrisler, attended a lecture in the 1970s, early on in her career on why there were no great women artists or novelists. The conclusion: women’s creativity declines when they are menstruating. This inspired Chrisler to devote her career to fighting menstrual stigma. In an era rife with sexism, adding PMDD to the DSM set off alarm bells.
Read More: A History of How Employers Have Addressed Women’s Periods
To further complicate matters, in the early 2000s, drug manufacturer Eli Lilly stuck its finger in the pie. Eli Lilly’s patent on its blockbuster drug Prozac, which treated depression, was set to expire and it’s share prices had tanked. The company desperately needed a new market that would buy Prozac.
Eli Lilly landed on PMDD as their next likely market. Early studies already suggested that Prozac could treat PMDD, but the problem was that experts were still debating whether PMDD belonged in the DSM as an official diagnosis at all. Undaunted, Eli Lilly embarked on a massive campaign to market Prozac to people with PMDD. It sponsored a round table discussion on Prozac’s effectiveness for PMDD, which found that at least 60% of patients with PMDD respond to antidepressants. It repackaged Prozac as “Serafem” a play on the word “seraphim”, the angels who guard the throne of God. If that wasn’t enough to drive home the point, they changed Prozac’s green and yellow pills to pink and purple. Finally, they rolled out a series of ads that suggested any woman who was feeling grumpy should consider medication. The ads didn’t distinguish between PMDD and PMS. Rather, they imply any sign of irritability in women should be treated.
This unleashed another wave of furor. Feminists were insulted—and rightfully so. The last thing the women’s movement needed was a drug companies suggesting a woman’s anger is a mental health condition. The media had a field day writing about drug companies “inventing” new diseases and marketing drugs without diagnoses. (Tragically, Prozac actually works on PMDD. Studies have found SSRIs like Prozac can relieve PMDD symptoms in up to twelve hours, even though it takes weeks to work for anxiety and depression.)
In some ways the feminists lost their battle. PMDD eventually did become a diagnosis in the DSM in 2013, nearly three decades after it’d been first debated in the ‘80s. In other ways, they won the war. Dr. Tory Eisenlohr-Moul, a premenstrual mood disorder researcher at the University of Illinois Chicago, estimates that the backlash around PMDD set care back by 10 to 15 years. She pointed out there’s been a chilling effect on the conversation around the link between menstruation and mood. Doctors are afraid to bring it up, because they don’t want patients to think they are sexist.
Yet, in reality, the biggest victims of the fight over PMDD’s existence are people who have PMDD and the people who love them. Today, thousands of people still suffer because they don’t know they have PMDD.
Tanya’s PMDD diagnosis changed her life. While she elected not to try medication, the diagnosis alone helped her understand her breakdowns, and helped her explain what was going on to family and friends. She decided to train in psychotherapy so she can help other people understand PMDD. “My tutor has been a counselor for 10 years and still hasn’t heard of PMDD,” she said. “I want to help people work through this pain.”
“}]]
PMDD, a menstrual mood disorder, impacts roughly 3 to 8% of menstruators. So why aren’t we getting people the help they need?
Uncategorized, Donald Trump
Health – TIME
PMDD, a menstrual mood disorder, impacts roughly 3 to 8% of menstruators. So why aren’t we getting people the help they need?
Read more
- Breaking News
- April 3, 2024
- 45 views
- 3 minutes Read
English News: Witness One Woman’s Margarita-Fueled Discovery of the Meaning of Fleetwood Mac’s Rumors—and Maybe Life Itself
English News: Witness One Woman’s Margarita-Fueled Discovery of the Meaning of Fleetwood Mac’s Rumors—and Maybe Life Itself
[[{“value”:”
One woman’s recent journey through Fleetwood Mac’s 1977 opus Rumors led to a truly wholesome moment online.
Raven Baxter, who goes by @ravenscimaven on X (formerly Twitter), shared on Tuesday night that she heard one of the hit songs from Rumors, “Go Your Own Way,” and was shocked to learn about the drama behind it and the whole album.
[time-brightcove not-tgx=”true”]
Rumors, which was an instant hit upon its release, came as multiple interpersonal relationships between Fleetwood Mac’s band members went sour: Stevie Nicks’ relationship with Lindsey Buckingham had ended; the group’s namesake drummer, Mick Fleetwood had learned his wife had cheated on him; and the late Christine McVie and John McVie divorced in 1976 after eight years of marriage, and still worked together on the album. All of this turmoil was channeled into what is regarded as one of the greatest albums of all time, sitting at No. 7 on Rolling Stone’s “500 Greatest Albums of All Time” list.
Baxter’s post went viral, and she continued to add to the thread as she listened to more of the album. “Wait is this WHOLE album two people in the band breaking up and fighting?!?!” she wrote.
Her posts about experiencing the great album for the first time endeared her to others, who delighted in her joy of discovery, and responded saying that they wished they could relive learning about the drama of Fleetwood Mac for the first time. The band trended on X on Wednesday, as users chimed in with suggestions for other Fleetwood Mac songs to listen to.
“If you love “Go Your Own Way” you have you to listen to “The Chain” *especially* after a couple of margaritas lol,” one person wrote. “that whole album is a trip. two couples breaking up and singing their feelings at each other,” another person wrote.
“}]]
A woman went viral for her tweets about discovering Fleetwood Mac and the drama that unfolded during the making of their 1977 album “Rumors”
Uncategorized, culturepod
Health – TIME
A woman went viral for her tweets about discovering Fleetwood Mac and the drama that unfolded during the making of their 1977 album “Rumors”
Read more
- Breaking News
- April 3, 2024
- 40 views
- 3 minutes Read
English News: Bird Flu Was Found in Chickens at the Largest U.S. Egg Producer
English News: Bird Flu Was Found in Chickens at the Largest U.S. Egg Producer
[[{“value”:”
The largest producer of fresh eggs in the U.S. said Tuesday it had temporarily halted production at a Texas plant after bird flu was found in chickens, and officials said the virus had also been detected at a poultry facility in Michigan.
[time-brightcove not-tgx=”true”]
Ridgeland, Mississippi-based Cal-Maine Foods, Inc. said in a statement that approximately 1.6 million laying hens and 337,000 pullets, about 3.6% of its total flock, were destroyed after the infection, avian influenza, was found at a facility in Parmer County, Texas.
The plant is on the Texas-New Mexico border in the Texas Panhandle about 85 miles (137 kilometers) southwest of Amarillo and about 370 miles (595 kilometers) northwest of Dallas. Cal-Maine said it sells most of its eggs in the Southwestern, Southeastern, Midwestern and mid-Atlantic regions of the United States.
“The Company continues to work closely with federal, state and local government officials and focused industry groups to mitigate the risk of future outbreaks and effectively manage the response,” the statement said.
“Cal-Maine Foods is working to secure production from other facilities to minimize disruption to its customers,” the statement said.
The company said there is no known bird flu risk associated with eggs that are currently in the market and no eggs have been recalled.
Eggs that are properly handled and cooked are safe to eat, according to the U.S. Department of Agriculture.
The announcement by Cal-Maine comes a day after state health officials said a person had been diagnosed with bird flu after being in contact with cows presumed to be infected, and that the risk to the public remains low. The human case in Texas marks the first known instance globally of a person catching this version of bird flu from a mammal, federal health officials said.
In Michigan, Michigan State University’s Veterinary Diagnostic Laboratory has detected bird flu in a commercial poultry facility in Ionia County, according to the Michigan’s Department of Agriculture and Rural Development.
The county is about 100 miles (161 kilometers) northwest of Detroit.
The department said it received confirmation of the disease Monday from the lab and that it is the fourth time since 2022 that the disease was detected at a commercial facility in Michigan.
Department spokesperson Jennifer Holton said Tuesday that state law prohibits the department from disclosing the type of poultry at the facility. The facility has been placed under quarantine and the department does not anticipate any disruptions to supply chains across the state, Holton said.
Dairy cows in Texas and Kansas were reported to be infected with bird flu last week — and federal agriculture officials later confirmed infections in a Michigan dairy herd that had recently received cows from Texas. A dairy herd in Idaho has been added to the list after federal agriculture officials confirmed the detection of bird flu in them, according to a Tuesday press release from the USDA.
Associated Press writer Corey Williams in Detroit contributed to this report.
“}]]
The Texas plant stopped production, and destroyed a flock, after bird flu was found in chickens there.
Uncategorized, healthscienceclimate, wire
Health – TIME
The Texas plant stopped production, and destroyed a flock, after bird flu was found in chickens there.
Read more
- Breaking News
- April 3, 2024
- 46 views
- 5 minutes Read
English News: Hormonal Birth Control Doesn’t Deserve Its Bad Reputation
English News: Hormonal Birth Control Doesn’t Deserve Its Bad Reputation
[[{“value”:”
Almost two-thirds of U.S. women of reproductive age use some kind of contraception, according to the latest federal data. And millions of them use methods that contain hormones, including birth control pills, intrauterine devices (IUDs), rings, implants, injections, and patches.
Although the specifics vary from method to method, hormonal birth control generally works by halting ovulation and/or changing conditions in the uterus or cervix to prevent pregnancy. And it works well: efficacy rates approach 100% when these methods are used correctly.
[time-brightcove not-tgx=”true”]
But hormonal birth control has a bad reputation. Many women are worried about how hormones like estrogen and progestin may affect their short- and long-term health, to the point that some are quitting birth control and choosing “natural” methods (which are often less effective) instead. A 2022 KFF survey found that about a third of reproductive-age women not currently using contraception avoid it because of concerns about side effects.
“They’re wonderful products, yet we maintain a cultural belief that somehow hormones are bad,” says Dr. Jeffrey Jensen, director of the Women’s Health Research Unit at Oregon Health and Science University. “That’s, in my opinion, simply not true.” (Jensen has received consulting fees from pharmaceutical companies that make contraceptive products.)
Here’s what the research says about hormonal birth control and health.
The side effects of birth control
In the KFF survey, about a third of women using contraception said they currently experienced side effects such as weight gain, headaches, bloating, nausea, mood changes, and menstrual changes. While these issues are usually not severe enough to be medically concerning, they can have a significant impact on quality of life. Studies show that many women who stop using birth control do so because of side effects.
But, Jensen notes, birth control sometimes comes with positive changes as well. It can lessen issues like acne, heavy or irregular periods, and menstrual cramps.
Is birth control linked to cancer?
There is research to suggest that women who use hormonal birth control are at slightly increased risk of breast cancer and cervical cancer. That elevated risk seems to be temporary, though, dropping off after a woman stops using birth control.
And studies also suggest that hormonal contraception reduces the risk of developing other types of cancer, including ovarian, endometrial, and colorectal disease—and those protective benefits seem to last for decades, even well after someone has stopped using birth control.
Read More: Teens Are Taking More Reliable Birth Control
When it comes to cancer, the pros and cons effectively cancel out, says Lisa Iversen, an advanced research fellow at the University of Aberdeen in Scotland. In 2017, she co-authored a study on birth control pill users’ lifetime risks of developing cancer, which involved analyzing decades of health data from more than 46,000 women. “Overall,” she says, “we found a neutral balance when you compare the risks and benefits.”
Still, Iversen says it’s always smart to speak with a physician about your specific personal and family risk factors before starting a new prescription.
Does birth control cause cardiovascular issues?
Birth control pills that contain estrogen have been linked to an increased risk of blood clots and stroke. But some researchers have questioned the strength of the association between contraception and cardiovascular problems. The authors of a 2022 review of previously published research concluded that there is little high-quality evidence to prove that birth control causes serious health issues, including cardiovascular complications and cancer. In fact, some recent research suggests birth control pills may actually decrease a woman’s risk of developing heart disease or dying prematurely.
Read More: Mammogram Guidelines Are Still Controversial Among Doctors
People with specific risk factors for stroke or blood clots should speak to their physicians before choosing a contraceptive method. But overall, it’s important to keep potential drawbacks in perspective, says Dr. Elizabeth Kinsey, a complex family planning fellow at the University of California, San Francisco’s Bixby Center for Global Reproductive Health. Pregnancy and birth also carry significant health risks, particularly given the U.S.’s abysmal record on maternal mortality, she notes.
Further, Kinsey says, conditions like cancer and stroke are diagnosed relatively infrequently among women of childbearing age. So even if contraception slightly increases a woman’s risk of developing them, her overall risk still remains low.
What about IUDs and other forms of hormonal birth control?
IUDs have a complex past. The Dalkon Shield, a type of IUD that became popular in the U.S. in the 1970s, was eventually linked to health issues including infections and pelvic inflammatory disease, causing some lingering concerns about these devices. Modern IUDs, however, are designed differently and have a good safety profile.
Hormonal IUDs available in the U.S. also do not contain estrogen, only progestin, which should minimize concern about clots and stroke, Jensen says. Studies on IUDs and cancer suggest a mix of pros and cons, similar to those associated with birth control pills: a slightly elevated risk of breast cancer, balanced by reductions in the risk of endometrial and cervical cancer.
Read More: What Borderline Cholesterol Really Means
One recent study also analyzed the hormone used in the birth control shot, medroxyprogesterone acetate. It found that prolonged medroxyprogesterone acetate use may be associated with an increased risk of developing a type of slow-growing (and usually benign) tumor in the membranes around the brain and spinal cord. Hormones used in IUDs were not associated with that risk, the study found.
Kinsey says she’d like to see more research on lesser-used forms of contraception, like rings and patches. But based on the science currently available, Jensen says most people don’t have huge reason to worry about using hormonal birth control, although individual risks are worth discussing with a doctor.
“For the most part,” he says, “we should be looking [at the science] and celebrating.”
“}]]
Here’s what you need to know.
Uncategorized, Evergreen, Explainer, healthscienceclimate
Health – TIME
Here’s what you need to know.
Read more
- Breaking News
- April 2, 2024
- 52 views
- 7 minutes Read
English News: Trump Built His Brand Bashing Obamacare. Now It’s More Popular Than He Is.
English News: Trump Built His Brand Bashing Obamacare. Now It’s More Popular Than He Is.
[[{“value”:”
This article is part of The D.C. Brief, TIME’s politics newsletter. Sign up here to get stories like this sent to your inbox.
A decade and a half ago, the Affordable Care Act set the stage for Donald Trump’s White House victory. The conservative backlash to Democrats’ massive and agenda-setting health care proposal was so strong that it gave rise to a newly empowered far-right faction in Congress, inspired a whole generation of angry political neophytes, and almost made Barack Obama a one-term President. Now, a solid 14 years later, those same rabble rousers seem to have convinced Trump, who spent years raging against the law informally known as Obamacare, that it might be good politics, if not also good policy.
[time-brightcove not-tgx=”true”]
It may be hard to remember now but Trump built his 2016 campaign on the twin cornerstones of the false and racist claims that Obama was not born in the United States and an unflinching scorn for Obamacare. He rarely passed up an opportunity to decry the law as a “disaster” or proclaim that it “sucks,” and repeatedly said a new effort was just “two weeks” away. As recently as a few months ago, he was vowing to destroy it if granted a second term. “We should never give up!” he declared in a Truth Social post in November.
A funny thing has happened in the last few years, though. Obamacare’s popularity has grown as more and more Americans interact with a health care system fundamentally rebooted in bite-sized pieces, and the potency of the hatred toward the Obamas has faded. (Some ugly comments, however, continue to crop up.) The result is the jabs against the 44th President’s legacy-worthy legislation no longer land with the same thwack, crackling barely as a thud.
Now, in 2024, it seems Obamacare will not be detonating, but maybe even stand to be firmed up if Trump wins a return to the White House. In a new series of messages, the former President is telling voters… Well, here is one of his social media musings in all of its glory:
I’m not running to terminate the ACA, AS CROOKED JOE BUDEN DISINFORMATES AND MISINFORMATES ALL THE TIME, I’m running to CLOSE THE BORDER, STOP INFLATION, MAKE OUR ECONOMY GREAT, STRENGTHEN OUR MILITARY, AND MAKE THE ACA, or OBAMACARE, AS IT IS KNOWN, MUCH BETTER, STRONGER, AND FAR LESS EXPENSIVE. IN OTHER WORDS, MAKE THE ACA MUCH, MUCH, MUCH BETTER FOR FAR LESS MONEY (OR COST) TO OUR GREST AMERICAN CITIZENS, WHO HAVE BEEN DECIMATED BY BIDEN, HIS RECORD INFLATION, BAD ECONOMY, AFGHANISTAN CATASTROPHE, AND JUST ABOUT EVERYTHING ELSE. CROOKED JOE BIDEN IS, BY FAR, THE WORST PRESIDENT IN THE HISTORY OF THE UNITED STATES! MAGA2024
This typo-laden turnaround—if that’s what it in fact is—was not always guaranteed. When the law was still taking shape, opponents convinced true believers that it would yield a rationing of health care services and perhaps even “death panels” that would do a cost-benefit analysis of treatments. Ultimately, after months of legislative hoop-jumping, the bill cleared Congress without a single Republican vote in support in March of 2010, and 34 House Democrats were against its final passage.
Polling immediately found the overall package to be an electoral clunker. A plurality 44% of voters held an unfavorable opinion of it in May of 2010, and those numbers didn’t really move all the way through Election Day that November, when Democrats suffered a seven-seat net loss in the Senate and dropped 63 seats in the House—the biggest wave since 1948. The unfavorable view of Obamacare was shared by 85% of Republicans that May, according to Kaiser Family Foundation polling. Months of Democratic explaining only shaved that number to 79% as voters headed toward the ballot box,
Put plainly: Obamacare might have been good policy, but it was lousy politics. The 14-month slog to pass the law left even its defenders with a bit of a chip on their shoulders. It wasn’t until fall of 2013 that people were able to sign up for private health insurance through the federal portal that was mired in glitches and bad P.R. For a long stretch there, Obamacare only brought ailments and not ointment. That’s where Trump picked up his initial instincts to seize on an often overlooked portion of the GOP’s base and feed the distrust.
And that tactic worked, at least until the upsides of the law kicked in. Over time, the polling got better. Parents of young adults realized their children could stay on their health plans as they got their careers going. The price tag for health care hasn’t exactly shrunk; the numbers tell the opposite story, actually. But the patient experience has gotten better even as medical bankruptcies and debts remain high. Still, there has not been a harsh rationing of care, and killing a regime that touches 45 million people—or roughly two-thirds of the size of all Social Security programs—is not a political winner.
That wasn’t necessarily the understanding when Trump and his nominal allies took over Washington in early 2017. Then, nixing Obamacare was atop their agenda. Trump unfurled executive actions—that later were rejected by the Supreme Court—and cajoled allies at the Capitol to move on his demands. But a revolt among moderates and GOP lawmakers in at-risk seats put that sect of the party on a collision course with the conservative ideologues. Party leaders pulled down the whole effort. Trump vowed revenge on those in the party who viewed as traitors.
“Obamacare unfortunately will explode,” Trump said in March 2017, trying his best to put shine on a loss. “It’s going to have a very bad year.”
Trump’s predictions of collapse proved faulty and now he’s hoping a national amnesia that has excused so many of his reversals carries into this realm. By this point, most Americans are numb to his flip flops; no one was truly surprised when Trump voiced support for TikTok not long after trying to ban it as President. But a TikTok ban was not integral to Trump’s political brand. For years, opposition to Obamacare was, almost as much as his support for a border wall.
It seems Trump has finally wised up to the fact that the health care law—while far from perfect—is doing good work for millions of Americans, perhaps becoming as sacrosanct as Social Security. The Supreme Court has repeatedly rejected efforts to scrap the law. Kaiser’s polling has 59% of Americans holding a favorable view of the Affordable Care Act, including 33% of Republicans. One report, released March 22, shows 45 million Americans benefiting from some aspect of the law. The days of “repeal and replace” seem to have faded as Trump finally realizes that even the law’s loudest critics lack a backfill program.
Republicans have quietly been positioning their most vulnerable members in this way, telling them that ending a program that has so quickly become enmeshed with day-to-day lives is a losing promise. Forty states, including some Republican-led ones, and the District of Columbia are participating in the Obamacare Medicaid expansion programs. Even weeks ago, as Trump was again thumping his ideas for canceling his loathed predecessor’s legacy law, Republican lawmakers were telling Trump he was on his own with no pals to “walk the plank” with him.
Biden seems eager to goad Trump to either defend his longstanding position or cop to a monumental flip-flop. In his State of the Union speech, the current President poked the former with plenty of pluck: “My predecessor, and many in this chamber, want to take those prescription drugs away by repealing the Affordable Care Act. I’m not going to let that happen. We stopped you 50 times before, and we’ll stop you again.”
For his part, Trump seems to finally realize the 51st time could be the most consequential to him yet: his own campaign this fall. So strong is his desire to reclaim power (and perhaps shut down some federal prosecutions against him), he will set aside more than a decade of anti-Obamacare language with barely a blink.
Make sense of what matters in Washington. Sign up for the D.C. Brief newsletter.
“}]]
“I’m not running to terminate the ACA,” Trump said in a typo-laden post.
Uncategorized, Donald Trump
Health – TIME
“I’m not running to terminate the ACA,” Trump said in a typo-laden post.
Read more
- Breaking News
- April 2, 2024
- 52 views
- 6 minutes Read
English News: The Perks of Being a Sociopath
English News: The Perks of Being a Sociopath
[[{“value”:”
“Don’t take things personally,” my professor warned my class. “Therapists have a responsibility to compartmentalize social emotions like shame and guilt. Try to ignore them,” he added. “What a patient is feeling toward you is not about you.”
It was day one of Clinical Practicum, a graduate-level psychology course meant to teach us how to work as clinicians. In addition to practical skills like assessment and treatment methods, we were introduced to the concept of transference, the inevitable unconscious process of patients redirecting their feelings onto their therapists. Negative transference was something that evidently contributed to a great deal of clinical burnout, as many therapists have a difficult time separating themselves from the emotions layered upon them by those they’re counseling.
[time-brightcove not-tgx=”true”]
“What’s the benefit in ignoring social emotions,” I asked.
“It allows you to observe your patient’s feelings,” he replied, “instead of absorbing them.”
That sounded like an advantage.
It wasn’t the first time I’d considered the upside of not connecting with guilt and empathy, social emotions which most people learn in early childhood. As a sociopath, these feelings come less easily to me than inherent emotions like joy and sadness. Dealing with this has certainly been a challenge, but I’ve also come to believe that some atypical traits of my personality type can be beneficial.
The American psychologist George E. Partridge suggested in 1930 that the term “sociopathy” be used to refer to the condition of the subset of individuals exhibiting atypical, antisocial tendencies. Current estimates indicate the prevalence of my personality disorder to be about 5% of the population. That means roughly 15 million people in America could reasonably be considered sociopathic. Yet any Google search on the topic will yield a who’s-who of serial killers and monsters. Like many sociopaths, I can assure you I’m neither. Though, I always knew something about me was different.
Read More: The Evolution of a Narcissist
I’ve never been able to internalize remorse. I started stealing in kindergarten, and my behavior worsened in elementary school. I had urges of violence and struggled with impulse control. By junior high, I was breaking into houses after school to relax. As my personality grew, so did my obsession with the word I’d heard used to describe it. “Sociopath.” Even as a teen I recognized some version of myself in its description. Except I never felt like a monster. And I didn’t want to be destructive.
My rebelliousness was not against parents, or teachers, or authority. It was more of a compulsion, my brain’s desperate way to jolt itself out of a suffocating apathy I had no way to convey to others. My struggle with feeling was like an emotional learning disability.
I knew I lacked empathy and wasn’t as emotionally complex as everyone else. But that was the point: I noticed these differences. This contributed to a unique type of anxiety, a stress associated with the inner conflict some believe compels sociopaths to behave in a way that is damaging. Unlike many on the sociopathic spectrum, I was fortunate to have a support system that enabled me to learn how to cope with this anxiety. That meant I was capable of both self-awareness and evolution, key milestones of emotional development that sociopaths supposedly can’t achieve.
It didn’t add up for me. Why did conventional wisdom, mainstream media, even college-level psychology courses, all pigeonhole such a significant portion of the population as irredeemable villains? There is nothing inherently immoral about having limited access to emotion. Millions of people spend billions every year in an attempt to free their mind and elevate their consciousness through meditation (or prayer) with the goal that is—for me, at least—my default state. Because it’s not what we feel or don’t feel. It’s what we do.
Of course, some sociopathic traits can be used destructively. I’m not trying to minimize the negative aspects of sociopathy or any of the anti-social personality disorders. But they can also be used constructively.
In pursuit of my PhD in clinical psychology, I spent thousands of hours counseling patients. My apathetic baseline enabled me to help people process their complex “big” feelings. I was able to act as an impartial container into which they could pour their deepest secrets, and I reflected no judgment about what they told me. I could better function as a neutral witness instead of a reactive participant because of my personality type. I recognized when negative transference occurred in my sessions, but it didn’t affect me the way it did other clinicians.
Secure in the knowledge that my psychological well-being isn’t something they need to protect, my friends and family, too, spare no details when looking to me for advice, support, or encouragement. This transparency allows me to be impartial when helping them confront often overwhelming feelings of indecisiveness, inferiority, shame, or guilt. Because I don’t experience those learned social emotions the way most people do, I can usually offer an insightful, helpful point of view.
I feel fortunate to have been spared the downside of these societal constructs. While research on sociopathy may still be sparse, there is no shortage of resources detailing the harmful effects of shame and guilt. From low self-esteem and a propensity toward anxiety and depression, to problems with sleep and digestion, the negative aspects of these emotions seem, to me, to far outweigh the positive.
Society would undoubtably fall to pieces if nobody ever felt bad about doing bad things. I get that. I acknowledge that “good” behavior is beneficial to society, just as I know there are tremendous benefits to living in a harmonious community. But, contrary to popular belief, it’s quite possible to make good choices even without the burdens of guilt and shame.
As someone whose choices are not dependent on these constructs, I like to think I can offer a helpful perspective. I’ve found that lending this point of view to people I care about lets them see their obligations through a more objective lens. This allows for healthy boundary-setting and self-advocacy, which can be just as helpful to overall well-being. Conversely, I’ve been able to adopt pro-social perspectives offered by others, enabling me to learn how they interpret things and better internalize empathy and compassion.
Like so many psychological conditions, sociopathy exists on a severity spectrum. For more than half a century we have identified sociopaths based solely on the most extreme negative behavioral examples, which only further alienates those living on the less extreme end of the scale. But there are millions of us who would prefer to peacefully coexist, who have accepted our own apathy, and have learned how to be valuable members of our families and community. We’ve learned to do this while living in the shadows. My hope is that one day we can step into the light.
“}]]
In a personal essay, Patric Gagne explores how sociopathic traits can be used constructively, instead of destructively.
Uncategorized, freelance
Health – TIME
In a personal essay, Patric Gagne explores how sociopathic traits can be used constructively, instead of destructively.
Read more
- Breaking News
- April 1, 2024
- 40 views
- 3 minutes Read
English News: A Person in the U.S. Tested Positive for Bird Flu
English News: A Person in the U.S. Tested Positive for Bird Flu
[[{“value”:”
In a rare case, the U.S. Centers for Disease Control and Prevention (CDC) confirmed on April 1 that a person in the U.S. has tested positive for avian influenza, also known as bird flu. Despite the positive test, however, the CDC says risk to the general public remains low.
Health officials have been tracking an outbreak of highly pathogenic avian influenza since a new variant emerged and began killing birds on multiple continents in 2020. Sixty-seven countries reported outbreaks in 2022, according to the World Health Organization (WHO), followed by another 14 in 2023. Human cases, however, remain rare. Only 11 infections resulting from the currently circulating strain have been reported globally since 2021.
[time-brightcove not-tgx=”true”]
Since January 2022, bird flu viruses have been detected among more than 82 million birds in the U.S., according to the CDC. More recently, mammals in the U.S.—including dairy cows and goats—have tested positive.
According to the CDC’s April 1 announcement, the person who tested positive had contact with cows in Texas presumed to have bird flu. Their only reported symptom was conjunctivitis-like eye redness. They were told to isolate and are recovering after being treated with flu antivirals, which seem to work against the virus, the CDC says. (Seasonal flu vaccines do not protect against avian flu, however.)
Read More: Is COVID-19 Still a Pandemic?
The U.S.’ last human case of avian flu was reported in 2022, after someone was exposed to infected poultry in Colorado. They went on to recover.
The CDC maintains that risk to the general public is low, although people who are in prolonged close contact with birds and livestock may be at increased risk of infection. The agency advises avoiding direct contact with sick or dead animals, as well as any materials that may have been contaminated by an animal infected with avian flu. People who may have been in contact with infected animals should be monitored for symptoms including eye redness, fever, cough, sore throat, congestion, muscle aches, fatigue, and shortness of breath. The disease’s severity can range from mild to fatal.
Food safety is not a major concern at this point, according to the U.S. Department of Agriculture (USDA). Poultry products are inspected for signs of disease before being made available for purchase, and dairy farms have been directed to destroy milk from infected cows. The pasteurization process also removes viruses from milk, and properly cooking eggs and poultry kills bacteria and viruses.
“}]]
Risk to the general public remains low, the CDC says.
Uncategorized, healthscienceclimate
Health – TIME
Risk to the general public remains low, the CDC says.
Read more
- Breaking News
- April 1, 2024
- 48 views
- 8 minutes Read
English News: Are Muscle-Building Supplements a Good Idea?
English News: Are Muscle-Building Supplements a Good Idea?
[[{“value”:”
Want to put on muscle? Who wouldn’t: It keeps you strong enough to do the things you love now, and it’s a great investment for later, since muscle improves bone mineral density and mobility as you age. People with more muscle mass have better outcomes when they’re sick, and quicker recoveries.
It’s hard not to be tempted by the powders, protein bars, and shakes promising to help. Whey, creatine, and branched-chain amino acids (BCAAs) are among the most popular of these. But what do they actually do, and who (if anyone) should take them?
[time-brightcove not-tgx=”true”]
Start with exercise
The first thing to know about muscle-building supplements is that they should not be your top priority. Resistance-training workouts should. These challenge your muscles, which is how to grow them.
“[You need] a stimulus greater than you’re used to…a load you aren’t used to carrying,” says Abbie Smith-Ryan, director of the applied physiology lab at the University of North Carolina at Chapel Hill. Most of us could stand to do more of it: only about a third of Americans do the recommended amount of muscle-strengthening exercise, according to the latest federal data.
For people who already do strength training, challenging your muscles might look like lifting heavier weights, shortening rest periods, or increasing the number of reps. The key is to “push your muscles to the edge,” says Elisabeth Barton, a muscle physiologist at the University of Florida. “Go to your limits.” This resistance challenge causes slight damage to your muscle, triggering a process called “regeneration,” in which cells activate and help grow new muscle fibers. As they repair the muscle, these cells multiply and fuse, increasing the overall size of the muscle. Resistance exercise also stimulates a cascade of growth signals that prompt muscle fibers to reinforce themselves, capillaries to expand the muscle’s blood supply, and DNA to make more proteins.
Read More: Why Walking Isn’t Enough When it Comes to Exercise
As long as you’re getting enough calories, this process works to increase your muscles. However, if you’re underfueling yourself, these muscle-challenging workouts can actually lead to muscle loss. When your body is forced to choose between growing your muscles and, say, feeding your brain, bigger muscles will always take the backseat. But for most people, the limiting factor for muscle growth is their workout, not a lack of nutrition, Smith-Ryan says.
Assess your diet
Foods can help you increase muscle mass, says Smith-Ryan. People who are exercising need between 1.4 to 2 grams of protein per kilogram of bodyweight each day (that’s 95 to 136 grams of protein for a person weighing 150 pounds). The majority of that will come from protein-rich foods like chicken breast, turkey, Greek yogurt, milk, and chickpeas.
However, “it is difficult to get enough macronutrients and the calories we need from whole foods,” since they can be time-consuming to prepare, Smith-Ryan says. “You are what you eat consistently.” And if a supplement helps you fuel your body consistently while you live your life, it might be a good option.
Whey
Whey can make up for some of what we miss in our diets. It’s considered a high-quality protein because it is absorbed quickly into the bloodstream and contains all nine essential amino acids—so named because the body doesn’t make them, so they must be consumed. (People can get all of the essential amino acids through a well-rounded diet.) It’s useful to have plenty of amino acids on hand—a kind of reservoir—when you train to support the regeneration process, Barton says.
Read More: Magnesium Supplements Are a Buzzy New Sleep and Anxiety Aid. Do They Work?
Using a whey product also boosts your protein without a lot of calories in the form of carbs and fats, Smith-Ryan says. Whey is fast and easy to eat on the go in the form of a smoothie or shake, making it a good option for busy people trying to get enough macronutrients. It might also be useful for people struggling to eat within the recommended window around a workout—15 to 60 minutes prior or 30 to 60 minutes after, Smith-Ryan says. Before or after a tough workout, a shake might be more appetizing than a chicken breast.
Creatine
Creatine doesn’t directly influence muscle growth, but it may still offer a little help. In the body, creatine is formed from amino acids and replenishes phosphocreatine, an important energy source for muscle cells.
“What it does benefit is the length of time you can train,” Barton says. Consuming it before a workout can help you train just a bit longer and eke out a few more reps. Since stimulus is the number-one muscle grower, creatine may help you put in more effective training sessions.
If you’re eating animal protein, you’re already making creatine. A teaspoon of the supplement creatine monohydrate contains the same amount of creatine as one pound of ground beef, Smith-Ryan says.
Vegetarians may have an even better response to creatine supplementation than omnivores since they tend to have lower creatine levels. One clinical trial found that vegetarians taking creatine showed a bigger increase in creatine stores, lean tissue, and exercise performance compared to non-vegetarians who took creatine.
However, if you don’t have a resistance training regimen just yet, creatine isn’t for you. “It doesn’t do anything for muscles without the added exercise,” Barton says.
Similarly, if you’re just starting out an exercise regimen, pass on creatine. This supplement is most useful for people who are already training consistently and looking for incremental improvement. If that’s not you, stick to the basics. Challenging workouts and proper fueling will be your best muscle builders.
BCAAs
BCAAs contain three essential amino acids: leucine, isoleucine, and valine. Unlike the other six essential amino acids, which are broken down in the liver, BCAAs are metabolized in the muscle. “When you see them in higher [amounts] in the blood, it’s a clear indication that muscles are breaking down,” Barton says.
Read More: What the Science Says About the Health Benefits of Vitamins and Supplements
Ads for these supplements suggest that taking them will replenish the muscle and prevent muscle loss, but there isn’t much data to support BCAAs in muscle growth. In fact, a 2017 review of the evidence called these claims “unwarranted.” “Ten years ago, the science seemed to show you needed BCAAs to build muscle, but what science shows now is you really need all the amino acids, not just BCAAS,” Smith-Ryan says.
Today, she recommends against a BCAA supplement. Instead, she advises, take a whey supplement for muscle growth or an essential amino acid (EAA) supplement, which contains all nine amino acids you need to get from food. EAAs are a good option if you don’t respond well to dairy and prefer to avoid whey protein. Some people like the taste of fruity EAA drinks over thicker whey protein shakes, Smith-Ryan says. It comes down to personal tastes.
How to take supplements
If you decide to incorporate supplements into your diet, it’s best to choose a product that’s been tested by a third-party organization like NSF, Banned Substances Control Group, or Informed Sport, Smith-Ryan says. She says that whey, creatine, BCAAs, and EAAs have “minimal cause for concern.” However, that’s not universally true for all supplements (which aren’t regulated by the FDA as strictly as drugs) that promise to boost muscle growth. And taking too much of anything can be problematic.
For instance, consuming large amounts of protein powder can cause digestive problems. This may be caused by a sensitivity to an ingredient in the powder, like dairy, soy, or gluten. It may take a few tries to find the protein powder that works best for you. Symptoms like diarrhea and bloating may also be a result of over-consuming sugar alcohols, a low-calorie sweetener used in many protein powders.
There have been some concerns that creatine causes dehydration, potentially by increasing the water content of muscle cells and thereby increasing the body’s water needs. However, this theory has not been supported in the research literature. Multiple studies have found that creatine actually improves hydration and reduces cramps. Still, multiple creatine brands advise customers to increase their water intake with creatine use. It’s always a good idea to read up on the product and take it as directed, Smith-Ryan says.
If you’re considering multiple supplements, remember that whey and EAA powders do the same thing, so you’ll only need one. But both can be safely taken alongside creatine, according to Smith-Ryan.
“}]]
You don’t need to take muscle-building supplements like whey and creatine. But they can help some people.
Uncategorized, Evergreen, freelance, healthscienceclimate
Health – TIME
You don’t need to take muscle-building supplements like whey and creatine. But they can help some people.
Read more
- Breaking News
- April 1, 2024
- 47 views
- 6 minutes Read
English News: What It Means if You Have Borderline High Cholesterol—And What to Do About It
English News: What It Means if You Have Borderline High Cholesterol—And What to Do About It
[[{“value”:”
Almost 25 million adults in the U.S. have high cholesterol, which puts them at a higher risk for a heart attack or stroke in the next decade. But a much bigger portion have what’s called borderline high cholesterol, an in-between place that’s not quite high, but not quite within a normal range.
Here’s what to know about borderline cholesterol.
What is borderline cholesterol?
[time-brightcove not-tgx=”true”]
High cholesterol is defined as having a total cholesterol number of 240 mg/dL or above. Someone has borderline cholesterol, meanwhile, when their total cholesterol is in the 200 to 239 range.
“We create these thresholds—which are admittedly somewhat artificial—to classify people so we can understand if we need to do further analysis or assessment to understand their risk for cardiovascular disease,” says Dr. Donald Lloyd-Jones, past president of the American Heart Association and a professor of cardiology and the chair of preventive medicine at Northwestern University Feinberg School of Medicine. There’s some flexibility: Some people may be completely healthy with a total cholesterol level of 235, while others could be at risk at 205. It depends on a person’s other risk factors. But broadly speaking, these thresholds help doctors make decisions about patient care.
People with total cholesterol levels below 200 tend to have a lower risk of developing heart disease, while those over 240 have a higher risk. Those who land from 200 to 239 are somewhere in the middle, Lloyd-Jones says.
Read More: How Stress Affects Your Heart Health
Cholesterol levels in this middle category aren’t automatically dangerous, but they do put you at a greater risk of developing high cholesterol, says Dr. Daron Gersch, a family physician with CentraCare Hospital in Long Prairie, Minn. And if you spend enough time in the borderline category, the effects can add up. People who had borderline high cholesterol for 11 to 20 years had twice as high a risk of developing heart disease compared with people who had high cholesterol for 10 years, according to research published in 2015 in Circulation.
“The analogy that I use is we are marinating our arteries in these cholesterol particles for our entire lifespan,” Lloyd-Jones says. “The more we marinate, the greater the chance that we form plaques. People who have very high levels for a short period of time are at risk of forming plaques, but even people who have modest levels for a long period of time can form plaques.” Those plaques build up and get inflamed over time, leading to heart attacks and strokes.
The type of cholesterol matters
Total cholesterol levels don’t paint the whole picture. What’s most concerning are your levels of low-density lipoprotein or LDL cholesterol, sometimes called “bad” cholesterol, says Dr. Ann Marie Navar, associate professor of cardiology at UT Southwestern Medical School and co-author of the Circulation study. That’s because LDL is the type of cholesterol that builds up in the arteries. A healthy LDL level is less than 100.
High-density lipoprotein or HDL cholesterol, on the other hand, is sometimes called “good” cholesterol because it removes fats from your blood, Gersch says. A healthy HDL level is 60 or higher.
Read More: 7 Myths About Cholesterol, Debunked
“If your total cholesterol is elevated because of the HDL, then you might not be at higher risk and actually might be somewhat protected,” Gersch says, “so it’s very important to not only get your total cholesterol levels, but to make sure it’s broken down into the good and bad cholesterol.”
That’s why it may be more accurate to look at borderline high LDL cholesterol only, Navar says. LDL cholesterol that’s 160 or higher is considered high, while LDL cholesterol from 130 to 159 is borderline, according to the American Academy of Family Physicians.
This is a rough categorization and not a guarantee of heart problems to come. “LDL-related cholesterol risk is on a continuum—there isn’t a magic number above which you’re at risk and below which you are not,” Navar says. “The higher your LDL is and the longer your LDL is elevated, the more risk you accumulate over time.”
How to lower borderline high cholesterol
After reviewing your blood test results in the context of your medical history, your doctor will recommend the best course of action to get your cholesterol levels into a healthy range for you.
If you have borderline high cholesterol but you’re otherwise healthy and younger than 60, your doctor may recommend lifestyle modifications that can help lower your overall risk of developing heart disease. These might include getting to and maintaining a healthy weight, eating a balanced diet (and scaling back on starches, alcohol, and high-fat foods), quitting smoking, and getting regular exercise.
Read More: Your Brain Doesn’t Want You to Exercise
But if you have borderline high cholesterol—and two or more other risk factors for heart disease—your doctor will likely recommend cholesterol-lowering medications to keep your heart safe as long as possible, Gersch says. Those risk factors include high blood pressure, diabetes, smoking or exposure to secondhand smoke, being 60 or older, having a family history of heart disease, being sedentary, or carrying extra weight.
When to get your cholesterol tested
If those risk factors sound familiar, you should start getting your cholesterol tested around age 20. Men without heart disease risk factors can typically wait until 35, and women without these risk factors can wait until 45 to start regular cholesterol testing, Gersch says.
You’ll be retested every four to six years if your test results show your cholesterol is in the healthy range. But you can expect to have bloodwork done more regularly, and as often as annually, if your levels land you in the borderline or high categories or you have other heart disease risk factors.
Having borderline high cholesterol may mean it’s time to start some preventive measures, but it doesn’t mean a heart attack or stroke is inevitable—and your overall health and risk factors for future heart disease matter more than one specific number in your cholesterol panel.
“Is there really a difference between 199 and 201? No, there’s not,” Lloyd-Jones says. Rather, this is a generalized, population-wide relationship between cholesterol and heart disease risk that’s only one piece of the puzzle on the individual level. “These are kind of arbitrary barriers, but they help initially determine how aggressive and intensive you want to be.”
“}]]
It’s an in-between place that’s not quite high, but not quite within a normal range.
Uncategorized, Evergreen, freelance, healthscienceclimate
Health – TIME
It’s an in-between place that’s not quite high, but not quite within a normal range.
Read more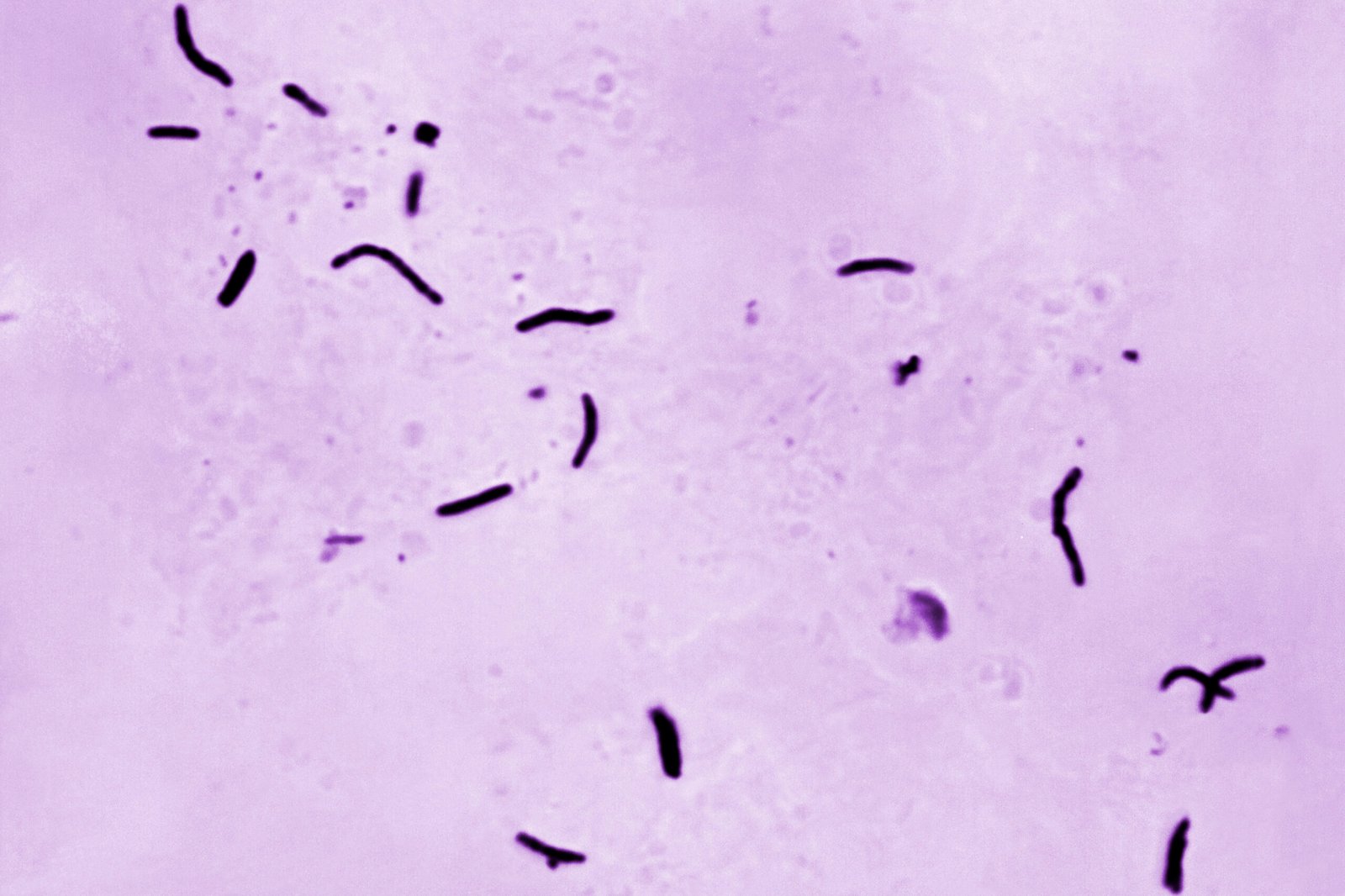
- Breaking News
- March 28, 2024
- 55 views
- 4 minutes Read
English News: Tuberculosis Is the Highest It’s Been in a Decade
English News: Tuberculosis Is the Highest It’s Been in a Decade
[[{“value”:”
NEW YORK — The number of U.S. tuberculosis cases in 2023 were the highest in a decade, according to a new government report.
Forty states reported an increase in TB, and rates were up among all age groups, the Centers for Disease Control and Prevention said Thursday. More than 9,600 cases were reported, a 16% increase from 2022 and the highest since 2013.
[time-brightcove not-tgx=”true”]
Cases declined sharply at the beginning of the COVID-19 pandemic, but have been rising since.
Most U.S. TB cases are diagnosed in people born in other countries. Experts say the 2023 number is in part a combination of a surge in TB cases internationally—the World Health Organization said TB was behind only COVID-19 in infectious fatal diseases worldwide in 2022. And there are also increases in migration and post-pandemic international travel.
But other factors are also at play, including other illnesses that weaken the immune system and allow latent TB infections to emerge.
CDC officials expected TB numbers would rise, but the 2023 count “was a little more than was expected,” said Dr. Philip LoBue, director of the agency’s Division of Tuberculosis Elimination.
Despite the jump, the number and rate of new TB cases each year remains smaller than it was in the past, and the U.S. has a lower rate of new TB cases than most countries.
Read More: Ticks Carry More Diseases Than Just Lyme
Tuberculosis is caused by bacteria that usually attack the lungs, and is spread through the air when an infectious person coughs or sneezes. If not treated properly, it can be fatal. In the late 1800s, TB killed one out of every seven people living in the United States and Europe. But the development of antibiotics and public health efforts succeeded in treating infections and tracking down those they infected, leading to cases falling for decades.
The new CDC statistics are not a count of how many people were newly infected in 2023, but rather of how many people developed a cough or other symptoms and were diagnosed.
An estimated 85% of the people counted in 2023 were infected at least a year or two earlier and had what’s called latent TB, when the bacteria enters the body and hibernates in the lungs or other parts of the body. Experts estimate as many as 13 million Americans have latent TB and are not contagious.
When the immune system is weakened—by certain medications or other illnesses like diabetes and HIV—the TB wakes up, so to speak. Nicole Skaggs said she was infected in 2020, but didn’t develop symptoms until 2022—after she got sick from COVID-19.
“Anything that can take out or lower your immune system can put you at risk,” said Skaggs, 41, a property manager in Bothell, Washington.
CDC officials called the idea that COVID-19 has played a role in increased reactivation of TB “an important question.” Scientists are still learning what causes latent TB to reactivate and “I would consider it an unknown at this point,” LoBue said.
“It’s too early to tell” what will happen to TB trends in the next few years, he also said.
There are TB vaccines being developed, and public health workers that were focused on COVID are now back to trying new approaches to preventing TB. New York City, which saw cases jump 28% last year, is hiring TB case managers and community health workers and increasingly using video monitoring of patients taking medications to keep treatment rates high, said Dr. Ashwin Vasan, the city’s health commissioner.
On the other hand, federal TB funding for state and local health department efforts has been flat, and one of the key antibiotics used against TB has been in short supply in recent years. Plus, drug-resistant TB infections have popped up in a fraction of cases.
“}]]
Forty U.S. states reported an increase in TB, and rates were up among all age groups.
Uncategorized, healthscienceclimate, wire
Health – TIME
Forty U.S. states reported an increase in TB, and rates were up among all age groups.
Read more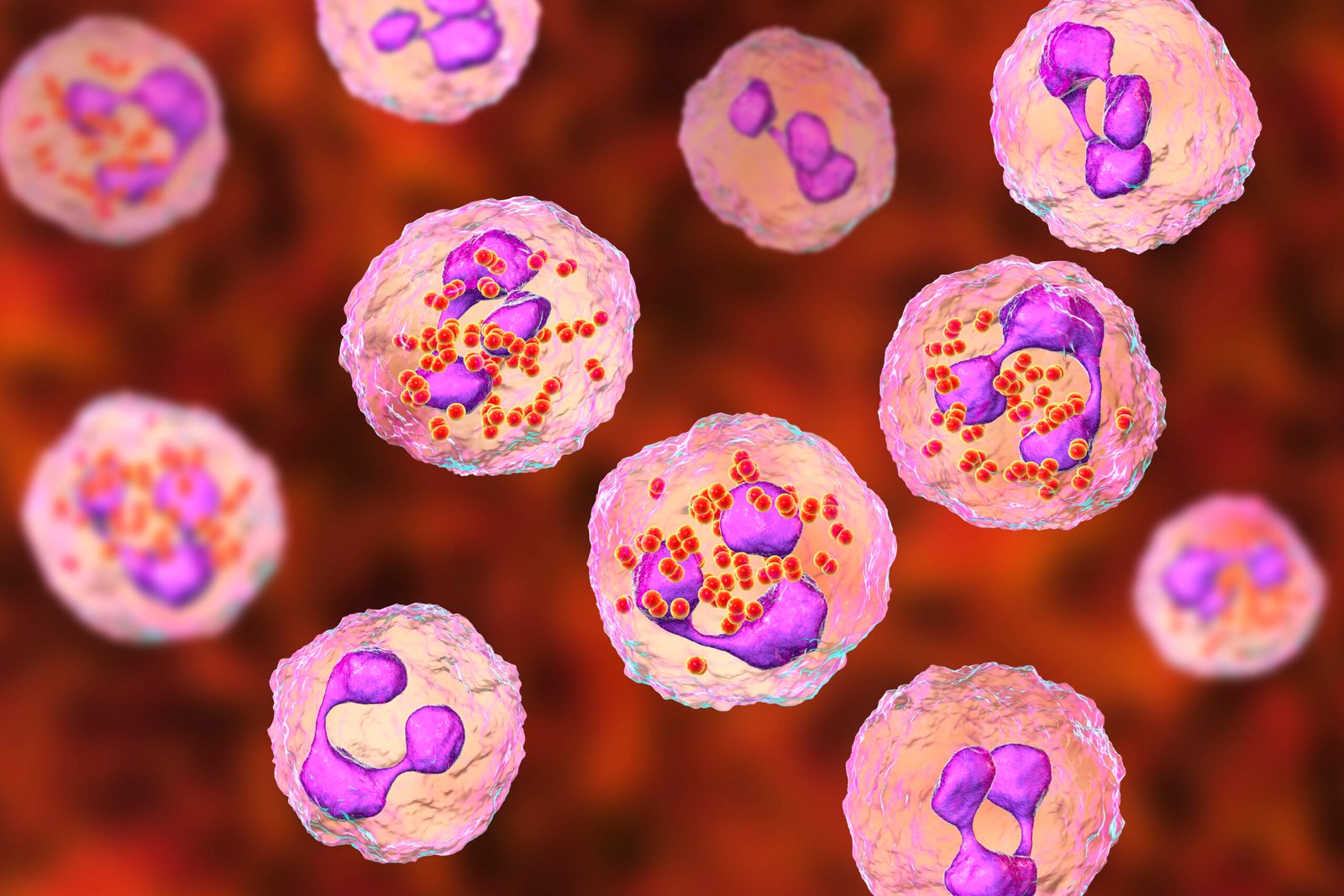
- Breaking News
- March 28, 2024
- 53 views
- 2 minutes Read
English News: A Rare Bacterial Disease Is Rising in the U.S.
English News: A Rare Bacterial Disease Is Rising in the U.S.
[[{“value”:”
NEW YORK — U.S. health officials are warning of an increase in rare bacterial illnesses than can lead to meningitis and possible death.
The Centers for Disease Control and Prevention issued an alert to U.S. doctors on Thursday about an increase in cases of one type of invasive meningococcal disease, most of it due to a specific strain of bacteria.
Last year, 422 cases of it were reported in the U.S.—the most in a year since 2014. Already, 143 cases have been reported this year, meaning infections appear to be on track to surpass 2023, the CDC said. Most of the cases last year did not involve meningitis, though at least 17 died. The cases were disproportionately more common in adults ages 30 to 60, in Black people and in people who have HIV, the CDC said.
[time-brightcove not-tgx=”true”]
The bacteria can cause a dangerous brain and spinal cord inflammation called meningitis, with symptoms that may include fever, headache, stiff neck, nausea, and vomiting. The bacteria also can cause a bloodstream infection with symptoms like chills, fatigue, cold hands and feet, rapid breathing, diarrhea, or, in later stages, a dark purple rash.
The infection can be treated with antibiotics, but quick treatment is essential. An estimated 10% to 15% of infected people die, and survivors sometimes suffer deafness or amputations.
There also are vaccines against meningococcal disease.
Officials recommend that all children should get a meningococcal conjugate vaccine, which protects against the rising strain, at around the time they enter a middle school. Since vaccine protection fades, the CDC also recommends a booster dose at age 16. Shots also are recommended for people at higher risk, like those in a place where an outbreak is occurring or those with HIV infection or certain other health conditions.
“}]]
Infections appear to be on track to surpass 2023, the CDC said.
Uncategorized, healthscienceclimate, wire
Health – TIME
Infections appear to be on track to surpass 2023, the CDC said.
Read more
- Breaking News
- March 28, 2024
- 42 views
- 6 minutes Read
English News: Why Walking Isn’t Enough When It Comes to Exercise
English News: Why Walking Isn’t Enough When It Comes to Exercise
[[{“value”:”
Walking is often thought of as a mere mode of transportation: a way to get from point A to point B. Few of us consider the fact that it’s one of the most fundamental, accessible physical activities a person can do.
What’s so great about walking?
Walking might not be as impressive as holding a plank or doing mountain climbers, but “it’s considered a bodyweight exercise, because your large muscle groups are working to move the weight of your body,” says Dr. Marie Kanagie-McAleese, a pediatric hospitalist at University of Maryland Upper Chesapeake Health and the leader of the Bel Air, Md. chapter of Walk With a Doc.
[time-brightcove not-tgx=”true”]
As you walk, “your quadriceps, hamstrings, calves—even your abdominals, biceps, and shoulders—are all using oxygen to contract,” says Ali Ball, an exercise physiologist and outpatient cardiac rehab/wellness coordinator at OSF HealthCare in Urbana, Ill. That also makes walking a form of aerobic exercise, she adds, which means it keeps your heart rate elevated for a sustained amount of time. One study published in the Journal of the American College of Cardiology found that 15 minutes of walking was as beneficial as five minutes of running.
From a physiological perspective, that’s a one-two punch of health benefits.
“First, walking improves the health of our cardiovascular system,” says McAleese. “With improved oxygen delivery to our organs, we see a decrease in the risk of heart disease, stroke, obesity, metabolic syndrome, diabetes, high blood pressure, and high cholesterol.”
Read More: Your Brain Doesn’t Want You to Exercise
Research bears this out. In a 2021 study published in JAMA Network Open, people who logged at least 7,000 steps per day had a 50 to 70%lower risk of early death, compared to those who walked less than 7,000 steps per day. Meanwhile, a 2023 meta-analysis published in the British Journal of Sports Medicine concluded that doing moderate-intensity physical activity—like brisk walking—for just 11 minutes a day is enough to lower the risk of diseases such as heart disease, stroke, and a number of cancers.
Plus, it’s the easiest way to counter the risk of a sedentary lifestyle, says McAleese. “Walking more throughout the entire day, even if you’re not doing it at a moderate-intensity level, is critically important,” since sitting too much increases the risk of getting—and dying from—many chronic diseases.
But is just walking enough exercise?
It can’t do everything. Federal physical-activity guidelines recommend at least 150 minutes of aerobic physical activity a week, plus two or more sessions of muscle-strengthening activities involving all major muscle groups per week. Both types of physical activity have to be of at least moderate intensity.
With a few tweaks, your walk can fulfill the first aerobic category. “Most people just don’t do it hard enough because they don’t think about it as exercise,” says Ball. If you’re used to a casual stroll, it’s easy to increase your intensity and get into that moderate range: You can increase the pace, walk on an incline, walk on a different terrain, or add weight via a vest or pack.
Read More: Forget 10,000 Steps. Here’s How Much Science Says You Actually Need to Walk
Not so much for the second category. “Walking does provide a low level of bodyweight exercise, but there are a lot of other muscle groups that we’re not really exercising when walking,” says McAleese. Strength training comes with a lot of additional health benefits, like lowering your risk of injury and improving mobility and flexibility.
How to make your walk count as a workout
Wearable devices have made mainstream the idea that everyone needs to hit 10,000 steps per day, but “that’s an arbitrary number not based in science,” says McAleese. A more important metric than steps, she says, is time. When it comes to the recommended 150 weekly minutes of moderate-intensity physical activity, “you can break that up however works for you,” she explains. “If you can only fit in 10 minutes here and 10 minutes there, it all counts.”
For walking to really qualify as “moderate-intensity” exercise, you need to be moving a little more intentionally than you would during a casual stroll from one meeting to the next. The guidelines consider walking briskly—where you could walk a mile in 15 to 24 minutes—to be moderate-intensity physical activity. That’s a purposeful, I-have-somewhere-to-be pace.
The best way to tell if you’re in that moderate-intensity range is the talk test. “If you’re able to speak in complete sentences and can carry on a conversation—but if you were to try to sing, you would become out of breath—that counts as moderate-intensity aerobic exercise,” says McAleese.
Read More: I Used ChatGPT as My Personal Trainer. It Didn’t Go Well
You can also check your heart rate. An approximate (but easy-to-remember) way to find your maximum heart rate is to subtract your age from the number 220, says Ball. During moderate-intensity exercise, your heart rate should be at about 50 to 70% of that maximum heart rate, according to the American Heart Association.
And to make sure you’re getting the most out of this type of physical activity, you also need to think about your form. (Yes, there’s proper form for walking.) “Focus on staying upright and keeping your abdominals engaged,” says Ball. Squeeze your butt, and let your arms swing naturally rather than exaggeratedly pumping them. Leaning forward, especially if you increase your intensity, can cause back pain.
For many people, embracing walking as exercise might just require a slight shift in perspective. “We focus a lot on scheduling exercise as a very specific activity that happens at a certain place at a certain time during our day,” says McAleese. “But we really should be expanding our definition of exercise to include all levels and amounts of physical activity that we perform throughout the entire day.”
“}]]
Walking is great, but it can only take you so far.
Uncategorized, Evergreen, freelance, healthscienceclimate
Health – TIME
Walking is great, but it can only take you so far.
Read more
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}